Travel With Us
"Life is either a daring adventure or nothing at all."
The smart Trick of How To Lower Health Care Costs That Nobody is Discussing
Costs, permitting state leaders to effectively leave out black people. [Myths about physical racial distinctions were utilized to validate slavery and are still thought by doctors today.] In 1945, when President Truman called on Congress to expand the country's health center system as part of a bigger healthcare plan, Southern Democrats acquired key concessions that shaped the American medical landscape for years to come.
But it likewise ensured that states managed the dispensation of funds and could segregate resulting centers. Expert societies like the American Medical Association barred black physicians; medical schools omitted black trainees, and many medical facilities and health clinics segregated black patients. Federal health care policy was developed, both implicitly and clearly, to exclude black Americans.
What's more, access to good medical care was predicated on a system of employer-based insurance coverage that was naturally difficult for black Americans to get. "They were rejected the majority of the tasks that provided coverage," says David Barton Smith, an emeritus historian of health care policy at Temple University. "And even when a few of them got health insurance coverage, as the Pullman porters did, they couldn't make usage of white centers." In the shadows of this exclusion, black neighborhoods developed their own health systems.

Black physicians and nurses most of them trained at one of two black medical colleges, Meharry and Howard established their own expert companies and began a concerted war against medical apartheid. By the 1950s, they were pressing for a federal healthcare system for all residents. [To get updates on The 1619 Job, and for more on race from The New York Times, our weekly Race/Related newsletter.] That fight put the National Medical Association (the leading black medical society) into direct dispute with the A.M.A., which was opposed to any nationalized health insurance.
The group used the exact same arguments in the mid- '60s, when proponents of nationwide medical insurance introduced Medicare. This time, the N.M.A. established a countermessage: Health care was a basic human right. Medicare and Medicaid were part of a wider plan that lastly brought the legal segregation of hospitals to an end: The 1964 Civil Rights Act outlawed segregation for any entity getting federal funds, and the new healthcare programs soon put every health center in the country because classification.
The Buzz on Why Single Payer Health Care Is Bad
Those who did not fit into specific age, work or income groups had little to no access to healthcare. Affordable Care Act brought health insurance to almost 20 million formerly uninsured adults - who is eligible for care within the veterans health administration. The most significant recipients of this boon were individuals of color, many of whom obtained coverage through the law's Medicaid growth.
Numerous states, the majority of them in the previous Confederacy, declined to take part in Medicaid growth. And numerous are still attempting to make access to the program contingent on burdensome brand-new work requirements. The outcomes of both policies have been unequivocal. States that expanded Medicaid saw a drop in disease-related deaths, according to the National Bureau of Economic Research.
One hundred and fifty years after the released individuals of the South first petitioned the federal government for basic healthcare, the United States remains the only high-income country in the world where such care is not ensured to every citizen. In the United States, racial health variations have actually shown as fundamental as democracy itself.
" Disparity is developed into the system." Medicare, Medicaid and the Affordable Care Act have assisted diminish those disparities. But no federal health policy yet has removed them.
World leaders have devoted to introduce universal health coverage by 2030 as part of the UN's Sustainable Advancement Goals. FEET writers go over the policies and developments in technology that could help bring this about.
The 10-Minute Rule for What Countries Have Single Payer Health Care
Author links open overlay panelMartinMcKeeMD1DinaBalabanovaPhD2SanjayBasuMD3WalterRicciardiMD4DavidStucklerPhD5Show moreOver the previous 50 years, health care has actually been making a growing contribution to population health in numerous nations. Yet its benefits are still rejected to many individuals worldwide. This short article describes the number of nations, both developed and establishing, have pursued the quest to achieve universal health care - how much would universal health care cost.
In Europe, it emerged from a belief in uniformity, a worry of transformation, and an altering view of the role of the state. In developing countries, development was more unpredictable, defined by debates about the price of universal healthcare, until it was recognized that operating health systems were vital to deliver advancement goals.
An analysis of development toward universal healthcare, combining a review of existing theories and brand-new empirical analysis, recognizes 5 elements as essential: the strength of arranged labor and left-wing parties, appropriate economic resources, lack of social divisions, weak point of organizations that might oppose it (such as organized medicine), and windows of chance.
global healthhealth systemsuniversal coverageRecommended articlesCiting short articles (0 )Copyright 2013 International Society for Pharmacoeconomics and Outcomes Research (ISPOR). Published by Elsevier Inc. All rights reserved.
Naresh Tinani loves his task as a perfusionist at a hospital in Saskatchewan's capital. To him, keeping an eye on client blood levels, heart beat and body temperature level throughout heart surgical treatments and intensive care is a "advantage" "the supreme interaction between human physiology and the mechanics of engineering." However Tinani has also been on the other side of the system, like when his now-15-year-old twin children were born 10 weeks early and fought infection on life support, or as his 78-year-old mom waits months for new knees amid the coronavirus pandemic.
The 8-Minute Rule for What Might Happen If The Federal Government Makes Cuts To Health Care Spending?
He's happy due to the fact that during times of true emergency, he said the system looked after his household without adding expense and cost to his list of worries. And on that point, few Americans can say the same. Prior to the coronavirus pandemic hit the U.S - how did the patient protection and affordable care act increase access to health insurance?. full speed, less than half of Americans 42 percent considered their health care system to be above average, according to a PBS NewsHour/Marist poll conducted in late July.
Compared to individuals in many established countries, including Canada, Americans have for years paid far more for health care while staying sicker and dying quicker. In the United States, unlike most nations in the developed world, medical insurance is often connected to whether or not you have a task. More than 160 million Americans relied on their employers for medical insurance prior https://transformationstreatment.weebly.com/blog/drug-addiction-delray-florida-transformations-treatment-center to COVID-19, while another 30 million Americans lacked health insurance before the pandemic.
Numbers are still cleaning, but one forecast from the Urban Institute and the Robert Wood Johnson Structure suggested as numerous as 25 million more Americans ended up being uninsured in current months. That research study suggested that countless Americans will fall through the cracks and may stop working to enroll for Medicaid, the nation's safety net healthcare program, which covered 75 million individuals before the pandemic.
Evaluate just how much you understand with this test. When people dispute how to fix the damaged U.S. system (a particularly common discussion during governmental election years), Canada usually turns up both as an example the U.S. ought to appreciate and as one it should prevent. During the 2020 Democratic primary season, Sen.
The Best Guide To Why Is Free Health Care Bad
In a recent governmental argument, one prospect specified several times that affordable health care is a right. With the emphasis on affordable, one is delegated consider in what contortion of economic reasoning can the government make anything more affordable. History is riddled with clear proof that federal government misshapes markets, making preferred products and services scarcer and greatly less budget-friendly.
Unfortunately, numerous are proposing greatly more government participation in the healthcare market. This varies from a public option to a single payer system. Those new federal government programs aside, the current federal government advancement in healthcare has been steadfastly metastasizing out of control. Federal government overreach in health care begins with the horribly misnamed Affordable Care Act.
Those whose hidden interest was government control of healthcare were excited to indulge this economic fallacy. Mandates drive costs up, not the other method around. What occurred was insurance coverage has actually become less cost effective, though more subsidized, and expenses have actually increased considerably. Even more, the ACA exacerbates the wearing down meaning of medical insurance as real insurance coverage.
Some Ideas on Western Societies: You Should Know
Those who then still can not manage healthcare can be subsidized by the federal government. There is little logic in transforming the whole healthcare system into a government-controlled program when just a portion of the population is in need of helpespecially as costs fall with a lowered federal government role. But the federal government intrusion into the health care marketplace is more insidious than the ACA.
Its immense damage to the market is a one-two punch: taxpayers suffer a huge opportunity expense by forcibly paying into a failing system and customers are pushed even more from making actual choices. The opportunity cost is simple to compute. Take the amount that both a worker and company paid in Medicare taxes over a lifetime of work.
Use a conservative mix of 50 percent in US equities and half in US government bonds. At 65, or whatever retirement age an individual picks, that account will almost certainly be multiples greater than what the government will administer. And the consumer would be choosing where and how to invest it.
A Health Care Professional Is Caring For A Patient http://titustljd187.lucialpiazzale.com/getting-my-with-respect-to-a-worker-s-health-care-coverage-to-work Who Is About To Begin Iron Dextran Can Be Fun For Everyone
In a market, the further the distance between the payer and the customer, the higher the distortion in the rate level. When the government makes healthcare decisions there is less incentive for consumers to manage cost and for manufacturers to lower expenses and innovate. The existing system of insurance coverage propagates a discrepancy in between individuals who get the healthcare, and those who pay for it.
The expense of a see to an emergency clinic is not inflated because of the uninsured who visit, but rather because essentially nobody who goes to actually pays the bill straight. This, of course, extends well beyond Medicare and government programs which amount to around half of all health care expenses.
Our tax system forces consumers to take part in insurance coverage plans that are not likely ideal for them and are not actually insurance coverage at all however rather a system that moves spending choices far from the real customer. Despite whether one thinks that economical health care is a right, it is clear that affordability and degree of government intervention are negatively correlated.
About Why Doesn't America Have Universal Health Care
The market is painfully misshaped, and the American people have less healthcare because it is less cost effective then it ought to be. As citizens reclaim control over their health care costs, expenses will be contained, and health care ends up being more inexpensive. what is fsa health care. As health care becomes more economical, its intake and quality increase.
The ACA needs to be rescinded. Medicare requires to be reformed. Health savings accounts need to be expanded. Government requires to leave the market. Health care decision making requirements to go back to individuals.
Possibly the United States health care system isn't that bizarre after all. Compared to peer nations, the United States sends out individuals to the healthcare facility less typically, it has a smaller share of professional doctors, and it offers people about the exact same variety of hospitalizations and medical professionals' visits, according to a brand-new research study.
Unknown Facts About How Does Culture Affect Health Care
If you have actually been listening to numerous of the typical stories that seek to discuss Alcohol Detox the high costs of America's health system and the country's reasonably low life span, those outcomes might amaze you. Analysts are fond of describing the system as wasteful, with a lot of clients getting too many services, driven by too many specialist doctors and too couple of social supports.
The paper, conducted by a research study group led by Ashish Jha, put together in-depth information from the healthcare systems of the United States and 10 other rich industrialized countries, and attempted to check those hypotheses. The group consisted of nations with single-payer healthcare systems, like Britain and Canada, and countries with competitive personal insurance markets, like Switzerland and the Netherlands.
Jha, the director of the Harvard Global Health Institute, said he pertained to the job with a sense of the conventional wisdom about how the United States varied from its peers. However, after putting together the data from the nations' health ministries, he altered his mind about a variety of crucial presumptions.
The Definitive Guide for How Much Does It Cost For Home Health Care?
But the research, he stated, didn't match his expectations. "I've been taking a look at other nations and seeing there's a great deal of fee-for-service in other countries, and other countries are dealing with overutilization."When it came to many of the procedures of health system function, the United States was in the middle of the pack, not an outlier, as Dr.
Many analysts have actually required the country to shift its doctor training away from specialized care and towards more medical care medication, for instance. But the study found that 43 percent of U.S. medical professionals practice primary care medicine, about typical for the group. It's often argued that clients in the United States use excessive healthcare.
The nation did rank near the top in its use of specific medical services, consisting of pricey imaging tests and specific surgeries, like knee replacements and C-sections. The data follow other proof that health care systems are beginning to assemble, as info and innovations spread around the world among doctors and administrators.
Rumored Buzz on Check out the post right here How To Take Care Of Your Mental Health
Even though other nations invest less than the United States, few believe they have actually discovered a way to tame costs forever. "I don't believe there's any of these countries where if you went and talked with them separately, they wouldn't say they're having a health care expense crisis," he said.

The systems tended to carry out much better than the United States on some steps and worse on others, with lots of tricks. Some professionals who reviewed the outcomes questioned the precision of all the paper's information points, which were numerous and drawn from a range of global sources. Dr. Jha acknowledged that the numbers might not be best but explained the effort as mindful and more detailed than previous contrasts.
The smart Trick of Which Of The Following Statements Is Not True About Costs In The U.s. Health Care
" Trump aides attack agency that will evaluate health costs's costs". Archived from the original on May 15, 2017. Date, S. V.; Young, Jeffrey (March 8, 2017). " White House Preemptively Attacks Congressional Budget Office On Obamacare Expense". Archived from the initial on March 13, 2017. Cornwell, Susan (March 17, 2017). " Republicans split, conservatives mad as healthcare overhaul inches ahead".
Retrieved March 17, 2017. Pear, Robert; Kaplan, Thomas (March 9, 2017). " G.O.P. Health Costs Clears 2 House Panels After Marathon Sessions". Archived from the original on March 9, 2017. Obtained March 9, 2017. Jacobs, Ben (March 9, 2017). " Republican healthcare plan approved by 2 Home panels, clearing significant hurdle". Archived from the initial on March 12, 2017.
" Trump Informs G.O.P. It's Now or Never Ever, Demanding Home Vote on Health Expense". Archived from the initial on March 23, 2017. " In Major Defeat for Trump, Press to Repeal Health Law Stops Working". March 24, 2017. Archived from the initial on March 24, 2017. Obtained March 24, 2017. Pear, Robert (March 7, 2017).
Archived from the original on March 12, 2017. Maureen Groppe, Democrats attempt to put brakes on Republican health care bill Archived March 9, 2017, at the Wayback Machine, U.S.A. Today (March 8, 2017). Rogers, Katie. " How the Health Care Vote Fell Apart, Action by Action". Retrieved March 24, 2017. Hensch, Mark.
The 6-Minute Rule for Which Of The Following Is True About The Health Care Latinos Receive?
Archived from the original on May 5, 2017. Obtained March 24, http://gregorypomu247.fotosdefrases.com/5-simple-techniques-for-what-does-cms-stand-for-in-health-care 2017. Sullivan, Peter; Hagen, Lisa; Hellmann, Jessie. " GOP leaders seek health care votes from contending factions". Retrieved March 24, 2017. " The Hill's Whip List: 36 GOP no votes on ObamaCare repeal strategy". Archived from the initial on March 21, 2017.
Sullivan, Peter; Wong, Scott. " Freedom Caucus, Trump reach 'arrangement in concept' on healthcare". Archived from the initial on March 23, 2017. Obtained March 24, 2017. Parnass, Sarah. " A held off health-care vote, a huge GOP embarrassment and no good choices ahead". Archived from the initial on March 24, 2017. Retrieved March 24, 2017.
" White House: Legislators will vote Friday on healthcare strategy". Recovered March 24, 2017. Davis, Julie Hirschfeld; Kaplan, Thomas; Pear, Robert (March 23, 2017). " Trump Tells G.O.P. It's Now or Never Ever, Demanding House Vote on Health Costs". Archived from the original on March 23, 2017. Recovered March 24, 2017. Wong, Scott; Lillis, Mike; Marcos, Cristina; Hellmann, Jessie (March 24, 2017).
Archived from the initial on March 24, 2017. Obtained March 24, 2017. Marcos, Cristina (March 24, 2017). " Home votes to begin argument on healthcare costs; six Republicans problem". Archived from the original on March 25, 2017. Retrieved March 24, 2017. Fabian, Jordan (March 24, 2017). " Ryan heads to WH to inform Trump on healthcare bill".
Excitement About What Is A Health Care Delivery System
Pear, Robert; Kaplan, Thomas; Thrush, Glenn (March 24, 2017). " In Major Defeat for Trump, Press to Repeal Health Law Fails". Archived from the original on June 14, 2017. Retrieved March 24, 2017. Wong, Scott (March 24, 2017). " House GOP abandons ObamaCare reverse effort in stunning defeat". Archived from the initial on May 9, 2017.

Zillman, Claire (March 14, 2017). " Trumpcare Could Signify the Beginning of the End for Guaranteed Maternity Coverage". Archived from the original on March 15, 2017. Bolling, Eric (March 14, 2017). " RyanCare is still ObamaCare. Here are five methods to begin over". Fox News. Archived from the initial on March 16, 2017.
" Republicare Edition". Archived from the initial on March 22, 2017. Recovered March 23, 2017. Newkirk, Vann R. II (March 6, 2017). " Is the GOP's Strategy 'Obamacare Lite'? Not Quite". Archived from the initial on March 22, 2017. Retrieved April 1, 2017. Holdman, Jessica (June 8, 2017). " ND unions rally for 'healthcare not wealth care'".
Archived from the original on June 9, 2017. Obtained June 15, 2017. Mental Health Doctor Garcia, Eric (June 1, 2017). " Cassidy Deals With Criticism on Healthcare at City Center". Roll Call. Archived from the initial on June 1, 2017. Retrieved June 15, 2017. " H.R. 1628: American Health Care Act of 2017 House Vote # 256 May 4, 2017".
How Which Of The Following Frequently Causes Health-care-associated Infections Of The Gi Tract? can Save You Time, Stress, and Money.
Archived from the original on May 5, 2017. (PDF). U.S. Legislature. Archived (PDF) from the original on April 28, 2017. (PDF). U.S. Legislature Committee on Energy & Commerce. Archived (PDF) from the initial on April 30, 2017. Fox, Lauren; Mattingly, Phil; Luhby, Tami (April 26, 2017).
Archived from the initial on April 26, 2017. Retrieved April 26, 2017. Jost, Timothy (April 25, 2017). " The MacArthur Amendment Language, Race In The Federal Exchange, And Danger Modification Coefficients". Health Affairs Blog. Archived from the original on April 26, 2017. Doran, Will (May 4, 2017). " Does the AHCA protect pre-existing conditions?".
Kaplan, Thomas; Pear, Robert (May 3, 2017). " With $8 Billion Offer on Health Expense, House G.O.P. Leader States 'We Have Enough Votes'". Archived from the original on May 4, 2017. Obtained May 4, 2017. Park, Haeyoun; Sanger-Katz, Margot; Lee, Jasmine C. (May 3, 2017). " What Republicans Changed in Their Healthcare Bill to Try to Get More Votes".
Retrieved May 4, 2017. " Last Vote Outcomes for Roll Call 256". U.S. Home of Representatives. May 4, 2017. Archived from the initial on May 4, 2017. " Additional info House Republicans pass bill to reverse and replace Obamacare". CNN. May 4, 2017. Archived from the original on May 5, 2017. Retrieved May 4, 2017.
A Biased View of What Is Health Care Policy
" House Passes Step to Repeal and Change the Affordable Care Act". Archived from the original on May 4, 2017. Recovered May 4, 2017. Soffen, Kim; Cameron, Darla; Uhrmacher, Kevin (May 4, 2017). " How your house voted to pass the GOP health-care bill". Archived from the original on May 5, 2017.
Lee, MJ; Luhby, Tami (June 22, 2017),, CNN, archived from the original on June 22, 2017, obtained June 22, 2017 Berman, Russell (June 26, 2017), " A New Charge for the Uninsured in the GOP Health-Care Expense",, archived from the original on July 4, 2017, recovered July 4, 2017 " McConnell delays healthcare vote while McCain recuperates from surgical treatment".
com. CNN (how much does medicaid pay for home health care). July 17, 2017. Archived from the original on July 16, 2017. Recovered July 17, 2017. Carney, Jordain (July 17, 2017). " Senate Dems: Usage ObamaCare repeal delay to hold public hearings". thehill. com. The Hill. Obtained July 17, 2017. Sullivan, Peter. " Senate votes to begin ObamaCare rescind argument". Retrieved July 25, 2017.
" Pence Breaks Tie as Senate Votes to Start Discussing Obamacare Repeal". Archived from the original on July 25, 2017. Recovered July 25, 2017. Weissmann, Jordan (July 27, 2017). " Would the GOP's "Skinny Repeal" Expense Really Wreck the Insurance Coverage Market?". Slate. ISSN 1091-2339. Archived from the initial on July 27, 2017.
How Has Obamacare Affected Health Care Costs Fundamentals Explained
Park, Haeyoun (July 27, 2017). " The "Skinny" Repeal Republicans Wish To Pass Would Leave Huge Numbers Uninsured". The New York City Times. ISSN 0362-4331. Archived from the original on July 27, 2017. Retrieved July 27, 2017. Pear, Robert; Kaplan, Thomas (July 27, 2017). " Senate Turns Down Slimmed Down Obamacare Repeal as McCain Votes No".
ISSN 0362-4331. Archived from the initial on July 28, 2017. Obtained July 28, 2017. " Amendment in the nature of an alternative to H.R. 1628, conversation draft LYN17709". Senator Graham. September 13, 2017. " Press Release: Graham-Cassidy-Heller-Johnson Background and Endorsements". Klein, Philip; King, Robert; Leonard, Kimberly (October 9, 2017). " Daily on Health Care: Trumpcare is pertaining to an association health insurance near you".
Not known Facts About What Does Cms Stand For In Health Care
I deal with the really real possibility of cancer repeating, with lifesaving treatment costing hundreds of thousands of dollars. I remain in remission, but life has no guarantees. As I struggled through the chemo-and-recovery cycle once again and again through the majority of 2017, I 'd examine the news every day to discover out what new lethal gimmick Republicans in the Senate were proposing.
Thanks to Sen. John McCain, we hung on, but by the slimmest of margins. I was living in Nevada at the time, and that September, my own senator then, Dean Heller, stepped forward and proposed yet another Obamacare repeal plan. To rub salt in the wound, Trump himself blocked me on Twitter after I criticized plans to rescind Obamacare, and he then tweeted hours later on in assistance of Heller's proposition.
But Republican politicians in Congress were not done with their health care sabotage. In early December 2017, the Republican-led Senate chose the Trump tax expense, which included a provision to gut the Affordable Care Act required. That vote set up the case prior to the Supreme Court that now threatens the whole Affordable Care Act.
I knew at the end of that year that I had to move to a state that had great state-level protections, simply in case Obamacare were revoked. Throughout the open registration duration, four states had the state-level defenses I was looking for. Therefore at the start of in 2015, I said goodbye to Nevada and ended up being a Coloradan.
So last summer season, I taken a trip on a bus across Colorado with other activists in search of Gardner, whose last public city center remained in 2017. Last fall, I even went to New york city City to attempt to speak with him face to face, without any luck. I have been to Gardner's workplaces numerous times to ask him to stop the legal attack on the ACA and to stand up for people with pre-existing conditions like me.
What Does A Health Care Administration Do Can Be Fun For Anyone
And make no mistake, there is no practical plan to replace Obamacare if it is overruled. Millions more might join our ranks as they recuperate from Covid-19. Without insurance coverage, many of us will die. Trump has likewise repeatedly claimed that he is trying to protect or "save" pre-existing condition protections while simultaneously assaulting the Affordable Care Act.
Trump has actually likewise consistently claimed that he is attempting to secure or "save" pre-existing condition protections while at the same time assaulting the Affordable Care Act and any system to make sure that people have comprehensive affordable protection. On Thursday afternoon, Trump revealed 2 executive orders on health care, one on pre-existing conditions and one on surprise billing.
Other Republican senators have actually taken Trump's lead. David Perdue of Georgia, Martha McSally of Arizona and Steve Daines of Montana have actually run TELEVISION ads declaring to secure people with pre-existing conditions regardless of their own voting records, and Thom Tillis, when one of the chief challengers of broadening Medicaid in North Carolina, is now quiet on health care.
Despite what they state on television about protecting the most susceptible, one by one the Republican senators are all getting in line behind Trump's Supreme Court candidate. We don't yet know who that is, however we can presume how she or he will vote on Obamacare. People with pre-existing conditions like me are again terrified of losing our insurance, this time in the midst of a pandemic.
Enough suffices. We are all healthcare citizens now. We'll see whether our wavering senators are healthcare voters, too. But these expenses provide far less protection than the existing ACA.Regardless, nearly every endangered GOP senator is participating this very same act. Here's an ad in which Cory Gardner of Colorado gets his mommy to inform you he'll protect individuals with pre-existing conditions. Here's another advertisement in which Joni Ernst of Iowa gets her sister to vouch for the same.
Excitement About Which Of The Following Is True About The Health Care Latinos Receive?
So motivating! Were it not for the reality that every one of them has voted to remove coverage for pre-existing conditions. As for the Trump administration, they're sounding the very same Browse around this site tune; when pressed, they will state: Well yes, we wish to rescind Obamacare. But it will be replaced with our incredible new health-care strategy! No, you can't see it.
However in another sense, Republicans in fact do have a plan. It's not the type of "strategy" that involves legislation or guidelines. Here's what it is: Nothing. This strategy might be more smart than you realize. Initially, it's essential to understand that even if Trump wins the election and Republicans hold the Senate, they have nearly no opportunity of taking back the Home.
So they will not attempt that again. Undoubtedly, in July 2017 when Sen. John McCain eliminated Obamacare repeal, much of the Republican politician Celebration released a sigh of relief. Republicans needed to attempt repeal due to the fact that they 'd promised it to their base for so long, but they had provided little idea to a serious replacement.
health-care system into chaos. The political effects would have been devastating. So the optimal strategy was to attempt to reverse the ACA, however stop working. And if they do not have total control of Congress in the future, it's not even worth the attempting part. Those senators run all those ads since they understand that the more the ACA is a concern, the worse it is for them; they're not attempting to win the argument, simply muddy the waters enough to lessen the damage they suffer.
Which they simply might, because at least some of the conservative justices such as Chief Justice John G. Roberts Jr. and Justice Brett M. Kavanaugh are clever adequate to understand how dangerous it is for their party. To be clear, if Trump is reelected, his administration will continue to use its regulatory and administrative power to undermine health security, specifically by attempting to push people off Medicaid.
The 6-Minute Rule for A Health Care Professional Is Caring For A Patient Who Is About To Begin Taking Cabergoline
In May 2018, Alcohol Abuse Treatment he boasted about "the strategies we have coming out, actually over the next four weeks." Twenty-four weeks later on having actually revealed nothing he stated, "We are working many strategies for health care. how much is health care per month." Last year, the president hedged on the timing of a healthcare plan, saying: "When the strategy comes out, which we'll be revealing you at the suitable time, it's much better than Obamacare.

Trump informed George Stephanopoulos of ABC that "we currently have the concept of the strategy" which he would "be announcing that in about 2 months perhaps less." That is essentially what he once again informed Mr. Stephanopoulos on Tuesday night, as Dr. Blaque firmly stood her ground. She told him she was born with sarcoidosis, an inflammatory illness that attacks numerous organs, "and from the day I was born, I was thought about uninsurable." When she asked if the Affordable Care Act's pre-existing conditions provision must "be removed," Mr.
Blaque cut in. Mr. Trump then duplicated that he would not "harmed pre-existing conditions" and turned the discussion to Democrats and President Barack Obama: "He said, you can have your doctor - what is home health care. You can have your strategy. Which turned out to be a lie, and he stated it 28 different times a minimum of." The exchange went viral.
D. facing the president delighted liberal Twitter. However the Fox News host Laura Ingraham, a staunch Trump backer, said he had been "assailed" in the town hall occasion and called the forum a "overall set up." In an interview Wednesday evening, Dr. Blaque, 57, said that while she relied on Medicaid as a younger woman, she was now guaranteed by the State of Pennsylvania, her company.
Because President Trump took office, Republicans have striven and accomplished a lot to enhance Americans' healthcare. Republican politicians have actually rescinded Obamacare taxes that hiked costs and stifled medical development, and they have actually helped get inexpensive generic drugs to the market much faster. Congress and President Trump likewise have actually protected America's youth from harmful tobacco items and have acted to more rapidly identify Alzheimer's disease and assistance households caring for enjoyed ones with this horrible disease.
What Is Health Care Policy Can Be Fun For Anyone
Republicans have actually not only taken actions to rescind the worst parts of Obamacare, but they have actually helped reduce the cost of drugs, increased innovation, and more sensibly invested taxpayer dollars. Republican politicians have actually likewise Alcohol Rehab Facility worked to help keep tobacco products out of the hands of youths and helped attend to the impact of the opioid epidemic on American families. how much does medicaid pay for home health care.
3% excise tax on the sales of medical devices Democrats consisted of in Obamacare hurt medical item innovation and task growth for the couple of years it was in location. Congress previously delayed the tax and successfully it in 2015. Rescinded Obamacare's Cadillac Tax: Last December, Congress likewise Obamacare's Cadillac tax, an excise tax on high-cost employer-sponsored strategies.
Reversing this tax supports the employer-sponsored protection that countless Americans rely on. Rescinded Obamacare's Health Insurance Tax: The health insurance tax consisted of in Obamacare raised premiums for elders and customers in the industrial market. this tax will decrease premiums for Americans starting next year and will enable companies to identify which health care plans fit the requirements of their employees.
The Facts About What Does Cms Stand For In Health Care Uncovered
" That was absolutely not true. In [the U.S.], lots of people wait and never ever get the care they need due to the fact that they're either uninsured or underinsured." Like Tinani's mom, lots of Americans have likewise postponed care amidst the pandemic out of issue that they might spread out or get exposed to the infection while being in a waiting space or standing in line for medications.
Department of Health and Human Services on Aug. 19 to enable pharmacists to train and qualify to administer vaccines to children ages 3 to 18, all in an effort to increase those rates and prevent mini-epidemics from spiraling amidst COVID-19. When the U.S. health insurance coverage industry smeared the Canadian system, they picked thoroughly picked points of attack, Potter stated.
They ignored to state Canadians were most likely to live after a cervical cancer diagnosis than Americans. In fact, Canadians delight in much better health results in general than Americans, from infant death Drug Rehab Center to life span. The COVID-19 pandemic belongs on that list, too. Canada has about one-tenth of America's population. Throughout the COVID-19 pandemic, Canada has seen many fewer cases and diseases, but the difference is not proportional.
However cases are speeding up in the U.S., https://ameblo.jp/zandervccm624/entry-12657566280.html which has ended up being the international center for the infection, with approximately 6 million verified cases and 183,000 deaths or the equivalent of one in five COVID-19 casualties worldwide. "It's truly discouraging to have to divert so much political energy towards what must be a no-brainer." One strength of the Canadian system to shine through throughout the pandemic is that everybody is guaranteed, Martin said.
Health centers deal with a single insurance company, she said, and that implies care is better coordinated throughout organizations. "Anybody that requires COVID care is going to get it," she stated. Dr. Ashish Jha, who has actually directed the Harvard Global Health Institute and now serves as the dean of the Brown University School of Public Health, has a somewhat various take.
and Canada present "a reflection that has absolutely nothing to do with the underlying health system" but rather reflects leaders and their political will and priorities. While America's health care system is among the world's best in terms of innovation and technology, Jha said that U.S. politicians have actually revealed themselves to be reluctant to trade off short-term pain of lockdowns and task losses for a long-term public health crisis and financial instability.
They also didn't ramp up testing quickly enough to efficiently keep an eye on when and where break outs would take place and repeatedly weakened the public health community in its efforts to successfully react to the infection. He said leaders in the U.S. have actually not used a clear consistent message or definitive leadership to unite the country and get everyone moving in the same instructions.
5 Easy Facts About Why Is Free Health Care Bad Explained
" It's truly frustrating to need to divert a lot political energy towards what ought to be a no-brainer," Jha stated. "This is the time when everybody who requires to be evaluated, is tested everyone who needs to be taken care of is taken care of." Which starts with consistent access to effective healthcare, he stated. what is fsa health care.
gone into lockdown under coronavirus, Sen. Bernie Sanders revealed on April 8 that he had pulled the plug on his governmental run. A week later on he endorsed previous Vice President Joe Biden. After contests in 28 states and two areas, his path to winning the Democratic election had narrowed significantly in spite of an early edge.

His project has actually proposed offering "every American a brand-new option, a public health option like Medicare" to make insurance more cost effective. As Potter views COVID-19 rage in the U.S., the previous health care interactions executive stated Americans reside in "worry of having big out-of-pocket expenses without guarantee that we'll have our expenditures covered." With the variety of uninsured Americans nearly double what they were before novel coronavirus, according to some quotes, Potter said that is not sustainable.
response to the coronavirus pandemic was listed below average, if not the worst, on the planet. This pandemic could bring the nation to a breaking point, Potter said, pushing more Americans to require a health care system that goes beyond the reforms of the Affordable Care Act, which the Trump administration has actually consistently assaulted and attempted to dismantle.
" You will see this campaign resurface to attempt to frighten individuals far from change," he said. "It occurs whenever there is a substantial push to change the health care system - what countries have universal health care. The industry wishes to safeguard the status quo." There's no best health care system, and the Canadian system is not without flaws, Flood said.
In June 2019, New Democrat Party Leader Jagmeet Singh proposed broadening Canada's pharmaceutical drug coverage. The ultimate goal of these changes that have actually been debated in differing degrees for several years is to incorporate oral, vision, hearing, mental health and long-term care to develop "a head to toe health care system." And yet it is natural for Canadians to compare systems with their neighbors and simply "feel grateful for what they have." She states that sort of complacency has actually insulated Canada's system from additional enhancements that produce usually better outcomes for lower costs, as in the UK, the Netherlands or Switzerland.
Registration for Member States and Observers Member States are motivated to take part in the top-level conference, consisting of the multi-stakeholder panels, at the greatest possible level, and to think about consisting of in their national delegations agents such as parliamentarians, mayors and governors, representatives of civil society, including non-governmental organizations, indigenous leadership, community companies and faith-based organizations, academia, philanthropic foundations and the economic sector, with due regard to gender equity - how much does medicaid pay for home health care.
10 Simple Techniques For Who Is Eligible For Care Within The Veterans Health Administration
Missions/offices are required to send their registration requests by using the online system "eRegistration" offered through the eDelegate Portal at https://delegate. un.int. The deadline for registration to all top-level conferences during the top-level period of the 74th session of the General Assembly is. Observers of the General Assembly are likewise welcomed to be represented at the highest possible level.
Agents of Member States wishing to speak during the plenary segment are encouraged to send their ask for inscription to the list of speakers through the e-Speakers system, which will be accessible at https://delegate. un.int from, at 9:00 a. m. EDT, up until, at 5:00 p. m. EDT. An automatic e-mail acknowledgement will be sent out within one hour of receipt of ask for engraving.
Observers wishing to speak during the plenary segment are kindly asked for to engrave to the list of speakers through the Secretariat (vrastiak@un. org) by. PaperSmart Services will be readily available for the plenary segment. Delegations are kindly asked for to submit electronic versions of their statements for publishing on the PaperSmart website to papersmart@un.
The title and the date of the conference should be suggested in the subject line of the Addiction Treatment Delray email. Member States and Observers who can not deliver their statement within the timeframe of the plenary sector might likewise submit their statement to PaperSmart. Conversations in the multi-stakeholder panels are planned to be interactive in nature and there will be no pre-established list of speakers.
Some Ideas on What Is Fsa Health Care You Should Know
As an outcome, 67. 2% of Americans have private medical insurance, mostly from their employers. The federal government subsidizes personal health insurance through Obamacare. Another 37. 7% of Americans have government coverage. These consist of Medicaid, Medicare, Children's Medical insurance Program, and military protection consisting of the Veterans Administration. Only 8. 5% had no coverage at all.
Numerous democratic prospects promote universal healthcare under the title "Medicare for All." In 2018, health care cost 16. 9% of GDP. That was a shocking US$ 10,586 per Click to find out more person. About 28% of patients reported a wait time of more than four weeks to see an expert. That has to do with the same as Germany and Switzerland.
The infant death rate was 5. 6%, practically double that of Australia and Germany. The third leading cause of death was a medical error. Country Type % of GDP Per Capita Wait 4+ wks Infant Mortality Rate (2017) Australia 2-tier 9. 6% $4,798 22% 3. 0 Canada Single 10. 6% $4,752 56.
5 France 2-tier 11. 0% $4,600 49. 3% 3. 5 Germany Mandate 11 (what is a single payer health care system). 3% $5,550 11. 9% 3. 1 Singapore 2-tier 4. 9% $2,000 2. 2 Switzerland Required 12. 4% $7,919 20. 2% 3. 7 United Kingdom Single 9. 7% $4,193 29. 9% 3. 7 United States Private 18. 0% $9,892 4.
7 * Data collected from 2016. Other than for France, 2013. Sources for Table: % of GDP. Per Capita. Wait 4+ wks for specialist. Infant death rate. The need for universal health care started in 1948, the year the World Health Organization declared health care a standard human right. The United States was sluggish to desert its model based on company-sponsored medical insurance.
Hillarycare, led by First Woman Hillary Clinton, recommended handled competition. Medical insurance companies would compete to offer the best low-cost plans. The government would control the expenses of doctor costs and insurance coverage premiums. Medical professionals, healthcare facilities, and insurance provider lobbied to defeat it in Congress. In the 2008 presidential project, Senator Barack Obama detailed a universal strategy.
The Ultimate Guide To How To Take Care Of Mental Health
People could pick it or buy personal insurance coverage on an exchange. The federal government would expand Medicaid funding and include aids. In 2009, President Obama proposed the Healthcare for America Strategy. It would have provided Medicare for all who wanted it. That would have lowered healthcare costs by 1% each year.
It relied on compulsory medical insurance, however enables many exemptions. States do not need to expand Medicaid. Trump's tax strategy removed the required in 2019. Numerous 2020 governmental prospects propose Medicare-for-all universal health insurance. Americans would have no deductibles, copayments, or out-of-pocket costs. It would likewise cut doctors' administrative expenses due to managing the variety of insurance coverage plans available.
healthcare administrative costs are double that of Canada. For universal healthcare to work, everybody, consisting of healthy people, should pay premiums or extra taxes to pay for health care. This funds the security health blanket for all residents. Preferably, with a healthcare system under federal government regulation, everybody will have access to quality treatments at low expenses.
U.S. health care is not as inclusive as other developed nations. Instead, it has different models for targeted populations. Obamacare is the closest to universality the United States has actually ever implemented, but it falls brief due to the fact that of its lots of exemptions.
If you're uninsured, you're not alone. 719,000 Virginians under age 65 do not have health insurance coverage. There's assistance if you can't afford it or can't pay for needed medical care. Virginians without insurance coverage may be http://angelouivm425.jigsy.com/entries/general/how-what-should-a-health-care-worker-do-immediately-after-a-safety-violation-occurs-can-save-you-time--stress--and-money- qualified for Virginia's state-sponsored medical insurance programs (Medicaid or FAMIS), or totally free or decreased expense care.
Now, many grownups in Virginia are qualified free of charge or low-cost protection through Medicaid. Medicaid and FAMIS also cover eligible children and pregnant females. Open Registration to buy medical insurance on the Medical insurance Marketplace runs from November 1 December 15 each year. To see if you get approved for a Special Enrollment Period, click.
Fascination About Why Is Health Care So Expensive
Click for what you require to learn about health insurance coverage. You might have the ability to get free or decreased cost treatment and prescription medicines at your local complimentary center or neighborhood health center. At some websites, you may have the ability to acquire dental care or get assist with psychological health services, too.
A (Lock A locked padlock) or https:// suggests you have actually securely linked to the. gov website. Share sensitive information just on authorities, secure websites.
A (Lock A locked padlock) or https:// implies you've safely connected to the. gov website. Share sensitive info just on official, safe sites.

There are a variety of complimentary health as well as dental programs offered for low to moderate income households, the disabled and senior citizens to name a few. There are likewise free medical insurance strategies. They are provided by federal government companies, business, charities, clinics, and other companies. The services and programs noted below will assist you and your household get high quality medical or oral care that is entirely totally free of charge.
The Children's Medical insurance Program, which is typically called CHIP, is readily available for low to moderate income families. Candidates can be working, have an income, and still get care. Discover how teens can get help from CHIP healthcare program. Health Resources and Services Administration (HRSA) - This is a federal government company that is part of the U.S.
It is the primary Federal government company that is accountable for providing and enhancing access to healthcare services for people who are separated, uninsured, clinically vulnerable, or lower earnings. The company partners with medical companies throughout the country. Find out more on Health Resources and Services Administration. Free health insurance may be offered.
Excitement About What Is Universal Health Care
Options consist of Medicaid, specific charities offer coverage, CHIP (for children and teens) and others. Discover how to secure free health or dental insurance. Medical care for uninsured - A combination of state, federal government, and non-profit companies offer support to families that do not have medical insurance or that have actually limited protection.
The truth is that the uninsured can get totally free healthcare for their medical needs. Seniors and older adults - The elderly, older Americans, and seniors can apply to federal government medical insurance programs that focus website on their particular needs. This can include the most popular, such as Medicare, but there are lots of others.
Senior citizens can also get assist examining medical costs from services such as SHIP, which is a totally free medical insurance counseling service for Medicare patients. Find out more senior support programs. State and regional healthcare clinics - Lots of regional and state federal governments support a wide variety of health care clinics that provide free health care to homeowners.
Neighborhood clinics and healthcare centers are located in the majority of towns and cities. State laws ensure charity healthcare - Numerous states have laws in location that guarantee homeowners are supplied greatly marked down or complimentary healthcare from regional hospitals if they satisfy certain earnings requirements. The policies likewise ensure reasonable billing practices for services incurred.
10 Simple Techniques For When Is The Senate Vote On Health Care
We are dedicated to decreasing health variations, which means making sure all Americans have access to economical, quality healthcare. There is absolutely nothing more essential to pursuing the American dream than health." All of this history has absolutely nothing to do with insurance, however only with a fundamental human right to health care. After the very first case appeared in January, the government rapidly established a diagnostic test and has tested millions of individuals free of charge. Lots Of South Koreans have actually benefited from drive-through testing websites. The government designated specific health centers Alcohol Detox for COVID-19 clients and needed patients looking for other medical care to check out non-COVID-19 medical facilities.
Health-care system. The Australian system uses a mix of public and private insurance coverage. The universal public health insurance coverage program, Medicare, is moneyed by the federal government. It's typically considered budget friendly, however there are compromises: public hospitals, for example, have been known to become overcrowded, especially throughout health crises. About half of Australians likewise purchase private insurancewhich the federal government encouragesthough this percentage dips to about one-fifth at lower income levels.
In 2018, investing in health amounted to 9. 3 percent of Australia's GDP. Australians paid typically around $830 in out-of-pocket health costs in 2016. COVID-19 reaction. Likewise ranked amongst the highest nations for epidemic readiness and reaction, Australia has actually not been as hard-hit by the pandemic, reporting around 6,300 cases of the infection and just under sixty deaths by mid-April.
10s of thousands of healthcare facility beds and countless physicians and nurses were moved out of personal medical facilities and into public ones to relieve stress on the public system. The country has also had amongst the greatest rates of screening per capita, balancing ten thousand tests daily in late March.
Health-care system. Under the highly controlled Dutch system, individuals are needed to buy health insurance from private suppliers, though these typically operate as nonprofit companies. Practically all medical facilities likewise run as nonprofits. The market is dominated by 4 insurance corporations, accounting for about 90 percent of enrollees. The federal government covers much of the costs, financed through taxation.
Dutch residents pay fairly low premiums ($ 115150 monthly) and out-of-pocket expenses (roughly $600 each Addiction Treatment Delray year), and companies likewise make contributions. Those with lower incomes receive extra subsidies, and costs for children are completely covered. More than 80 percent of the population buys voluntary, complementary insurance coverage to cover benefits such as dental and eye care.
The 9-Minute Rule for A Health Care Professional Is Caring For A Patient Who Is About To Begin Using Betaxolol
Though analysts alert that health costs are rising faster than incomes, the system is hailed for its available, premium care. COVID-19 action. The Netherlands has a nationwide public health institute with guidelines in place for epidemics - how many countries have universal health care. Following the institute's recommendations, Prime Minister Mark Rutte's federal government implemented social-distancing procedures in March, however chose against a complete lockdown, arguing that a controlled spread of the virus could construct resistance.
Though the rate of transmission seemed slowing, authorities cautioned that hospitals' extensive care units could reach capacity. Personal locations, including a concert hall and hotels across the nation, have actually been become makeshift emergency situation centers to reduce tension on hospitals, which have had high rates of infection among staff.
Since April 6, the country's per capita testing was on par with that of the United States, but was far behind South Korea's. Health-care system. The United States, whose health system is a mix of personal and public sources, is one of the only high-income nations that has actually not achieved universal health coverage: around 8.
The 2010 Affordable Care Act needed most Americans to have insurance coverage, but that requirement was removed by President Donald J. Trump's administration in 2019. Personal insurance, whether employer-based or individually purchased, represent two-thirds of the marketplace, while the staying one-third of individuals are covered by public insurance plans including Medicare, Medicaid, and veterans' programs.

Americans invest far more on healthcare than citizens of any other OECD nation. People pay an average of $10,000 [PDF] yearly, and nearly 17 percent of U.S. GDP was invested in health in 2018. COVID-19 action. After the United States reported its very first coronavirus case in late January, the Trump administration prohibited travelers from China.

Regardless of being ranked as the most prepared for a pandemic, the nation did not ramp up capability in medical facilities or substantially boost production of medical materials. Some states, such as California, carried out early lockdown measures and had more success in suppressing the infection's spread. A preliminary diagnostic test created by the Centers for Disease Control and Prevention (CDC) proved to be defective, postponing screening nationwide for weeks and preventing health authorities from having a precise photo of the disease's spread.
Facts About Countries Whose Health Systems Are Oriented More Toward Primary Care Achieve Revealed
With numerous states dealing with lacks, Trump has used emergency situation powers to force private business to make ventilators for clients and masks for health-care employees. March 2020 legislation made coronavirus tests free, but costs for treatment differ.
UHC indicates that all individuals and neighborhoods get the health services they need without suffering monetary hardship. how much would universal health care cost. It consists of the complete spectrum of essential, quality health services, from health promo to avoidance, treatment, rehab, and palliative care. UHC enables everybody to access the services that address the most significant causes of disease and death, and guarantees that the quality of those services is excellent enough to enhance the health of the people who get them.
Attaining UHC is one of the targets the countries of the world set when embracing the Sustainable Advancement Goals in 2015. Countries that progress towards UHC will make development towards the other health-related targets, and towards the other goals. Good health enables kids to discover and adults to earn, assists people leave from poverty, and offers the basis for long-lasting financial development.
UHC is not just about health financing. It incorporates all parts of the health system: health service delivery systems, the health workforce, health facilities and interactions networks, health technologies, details systems, quality control mechanisms, and governance and legislation. UHC is not only about making sure a minimum bundle of health services, however likewise about making sure a progressive expansion of protection of health services and financial protection as more resources appear.
UHC is consisted of far more than just health; taking steps towards UHC suggests actions towards equity, advancement priorities, and social inclusion and cohesion. Many nations are already making development towards UHC. All nations can act to move more quickly towards it, or to preserve the gains they have currently made.
Moving towards UHC needs reinforcing health systems in all nations. Robust funding structures are crucial. When people need to pay the majority of the cost for health Mental Health Facility services out of their own pockets, the poor are frequently not able to obtain a number of the services they need, and even the abundant might be exposed to financial challenge in the event of serious or long-term illness.
Unknown Facts About A Health Care Professional Should Question The Use Of Metoclopramide For A Patie
You will need to complete the registration type to use this is not offered Drug Rehab online, so you will need to call the Rgie or check out a Rgie office to obtain one. If you check out a workplace in-person, you can complete the form during the exact same visit so long as you have the essential proof-of-identity paperwork with you.

Proof of home in Quebec can be shown by providing a copy of a domestic lease, deed of purchase for a home, or attestation from a company. Momentary employees, who can provide an immigration document showing their employer's name and specifying they may operate in Quebec for a minimum of six months, are also qualified for healthcare protection in Quebec - how to take care of your mental health.
Medical insurance in Saskatchewan is supplied by the Saskatchewan Health Authority. Long-term residents and eligible short-lived citizens transferring to Saskatchewan may be qualified for health coverage on or prior to the very first day of their third month after getting here in Canada. Copies of documents proving your legal privilege to be in Canada, residency in Saskatchewan, and identity needs to be supplied.
All medically necessary services, including both inpatient and outpatient services, are consisted of with Saskatchewan Health Card coverage. Saskatchewan likewise provides some supplemental services, consisting of oral services and prescription drugs, to advised individuals. Find out more about health care in Saskatchewan - which of the following are characteristics of the medical care determinants of health?. Yukon Health Care Insurance offers coverage for locals of the Yukon.
Brian Lindenberg April 16, 2012 In my last article for BenefitsCanada. com, I compared and contrasted the state of healthcare in this country at the time that the fundamental concepts for the Canada Health Act were developed (in 1961) and today. As the federal government is about to undertake a review of this legislation, it is necessary that all Canadians formulate a viewpoint on the future of our health care system.
Initially, a crucial recognition: the health care dispute is charged with emotion. Canadians from all strolls of life have different experiences with our health care system, and these kind our opinions. My own experiences with our system have been generally favourableothers I know have actually had completely difference experiences. Furthermore, there are those Canadians who are also health professionals working within the system who are constantly asked to do more with less.
Weighing each point of view is the next-to-impossible task put prior to the federal government as it develops a design template for Canada's health care system that will last another 50 years. So with this extremely crucial caveat, let's consider what currently works well within our existing healthcare system and what does not. Unlike in the U.S., no citizen of this nation is rejected access to health care based upon whether or not he or she can manage to pay.
Which Of The Following Represents The Status Of A Right To Health Care In The United States? Can Be Fun For Everyone
Universal healthcare defines us as Canadians. As soon as you are in the system, the requirement of care is excellent. For instance, health outcomes in the areas of cardiovascular illness and many forms of cancer are far much better than in the U.S., which recommends that we are doing lots of things right. Of course, the personnel words here are "once you are in the Drug Rehab Delray system." Clearly, reasonable access to care is a problem that this nation should deal with.
For every single dollar invested in healthcare funding, far less gets invested in administration than in nations such as the U.S. Our system is far from ideal, however in relative terms, it is not bad. Canada has among the most costly health care systems worldwide. We can want to many other nations to see remarkable health for less cash.
Health care choices are frequently made based on "political palatability" or what's acceptable to the voting public versus what makes good sense from a monetary sustainability perspective or in terms of health outcomes. The decision-making process is made complex and typically slow, and results in small incremental modification rather than basic change. We are likely at a moment where we require to ask the tough questionsbut the politics of decision-making will get in the method and we may not get to where we need to be.
The system has not stayed up to date with the demands and expectations of the patient. Our healthcare system is substantial and, for that reason, not very nimble. Although numerous provinces are attempting to change this, our system stays concentrated on acute and chronic careaddressing the issue once it becomes a problem. A lot of professionals concur that the focus needs to move to avoidance and health promotion.
The system has likewise not kept up with the altering face of disease and treatment. For example, physical health stays the main focus of the system Extra resources while mental disorder represents a considerable expense to the Canadian economy and society. Drug therapy is utilized extensively in the treatment of injury and illness, yet these costs fall mostly beyond the general public system.
Healthcare funding across the country is far from constant with access to care specified, in part, by your province of house. And this gap will just get larger as resource-rich provinces such are Alberta and Saskatchewan are able to invest more on a per capita basis than the other provinces.
So where to from here? A lot of the standard concepts embedded in the Canada Health Act still work. Nevertheless, this crucial piece of legislation needs to be updated to reflect the truths of today. The concepts of public administration and the standards for what is "clinically necessary" in specific need to be examined to guarantee that whether what was anticipated in 1961 still works today.
The Ultimate Guide To What Does A Health Care Administration Do
We can most likely all settle on the objectiveto develop a structure for a cost-efficient, efficient healthcare system that responds to the medical requirements of all Canadians. How we arrive goes through debate. But we do need to get there, and the debate requires to begin now.
The Canadian healthcare system has actually been a definite success considering that its intro in the country in 1967. The publicly financed healthcare system offers health services that are primarily free to Canadian citizens and handled and administered on a provincial and territorial level directed under the Canadian Health Act.
However, the general public funded healthcare system does not cover prescription drugs, home care or long-term care, prescription glasses or dental care, for that reason Canadian residents spend for these services either out of their pockets or through private medical insurance coverage and employer-sponsored plans. The health care system which is likewise called Medicare in Canada is provided to all residents and is not determined by the finances of individuals.
These education programs look for to make residents more aware, so they can avoid injuries and offer a more proactive method to basic health problems so that conditions are discovered previously thus minimizing their effect. These programs are fully funded by the Canadian federal government and go a long method in informing citizens of all ages and backgrounds.
The Canadian Medicare takes into consideration the needs of kids, handicapped citizens and the elderly. For senior citizens or veterans and disabled kids, there is a need for unique care and attention, and the healthcare system was created with this in mind. Canadian health insurance coverage is a national health program called Canada Medicare (public health insurance coverage).
The Ultimate Guide To What Countries Have Universal Health Care
Predominantly the underlying reasons for medical errors are; technical failures - how did the patient protection and affordable care act increase access to health insurance?. Hospitals are a typical setting for health center got conditions in part due to the fact that of the medically compromised state of many clients confessed to the hospital and high volume of care transactions and interventions that happen throughout a medical facility stay.
Hindsight predisposition occurs when the investigators work direct analysis makes the path to failure look as though it need to have been foreseeable or predictable, although this is not the case (how did the patient protection and affordable care act increase access to health insurance?). Frequently this determination is made without any evaluation of systems or procedures that might have contributed to the mistake.
Nevertheless there is no space for negligent behavior in the healthcare environment.is the procedure of the possibility that an event will happen. https://cashrokq084-12.webselfsite.net/blog/2021/03/23/how-many-countries-have-universal-health-care-things-to-know-before-you-buy is any activity that represents a possible threat. is a weakness. results in a compromise to functions, life or properties. are Health Center Acquired Conditions. is an unwanted result Mental Health Facility or incident, not expected within the regular course of care or treatment, disease procedure, condition of the client, or shipment of services.
is an unexpected incident including death or serious physical or psychological injury, or the risk thereof, unrelated to the natural course of a patient's health problem or underlying condition. Scope of the Threat Management Contextsa. Enterprise Threat Management (ERM): Comprehensive risk management of the company from leading down including b.
Medical staff (Such as; credentialing, privileging, task descrip-tion, staff member insurance coverage, trainings, medical coverage) d (how does the health care tax credit affect my tax return). Non-medical staff (Such as; task description, training, medical coverage) e. analysis, insurance coverage) f. Supervisory (Such as; organogram, Job descriptions, delegation of work) g. Task danger management (Such as scope, time, cost, human resources, functional, procedural, technical, natural and political) h.
Risk Management Information System (RMIS) Threat Management Details system (RMIS) is a computerized system utilized for information collection and processing, info analysis Secret Principles in Risk ManagementRisk manageorganized effort to identify, examine, and decrease, where appropriate, threat to patients, visitors, staff and organizational assets. Threat management in its finest form might be to use it in a pro-active way in recognizing and managing the risks.
health care experts to quickly understand the crucial concepts in risk management and implement them in the health care companies where they work. Received Date: April 12, 2016, Accepted Date: September 23, 2016, Published Date: October 03, 2016 - what does a health care administration do. * Corresponding author:.
6 Simple Techniques For What Is A Single Payer Health Care Pros And Cons?
The role of risk management in healthcare has actually come a long way over the years. However as dangers to the health Drug Rehab Facility care market multiplyboth in number and costsrisk management and danger managers require to be at the leading edge of the service. If not, healthcare companies can't grow, or possibly even make it through. what countries have universal health care.
This is a shift from the 1970s and 1980s, when risk managers were almost solely focused on clinical problems and lessening damages from the abundance of medical malpractice and expert liability claims being submitted throughout that time. Likewise problematic: They were essentially handling this single threat from their own separated departments And while isolated and unconnected risk management practices may have enabled health care organizations to survive the medical malpractice and expert liability storm 30 and 40 years ago, such practices are not sustainable in today's troubled healthcare environment where risks are more varied and complicated than ever in the past.
However doing so needs a broader technique to risk management, like Integrated Business Danger Management. Integrated ERM brings all threats from throughout the business together to figure out how they relate uncovering insights that have formerly been hidden within private silos. It focuses on organizational systems and procedures; tends to be proactive in nature, instead of reactive; and hinges as much on value development as it does run the risk of mitigation.
Such advantages do not come without work, however. For beginners, risk supervisors can finish an organization-wide danger assessment, taking into account the threat domains established by the American Society for Healthcare Danger Management (ASHRM). The threat domains consist of operational, human capital, innovation, hazard, tactical, clinical/patient safety, legal/regulatory and monetary dangers. From there, you will need to determine areas of focus that need enhancement, which will necessitate access to information that can effectively highlight difficulty spots or potential success storieslike decreases in worker injuries or workers' payment expenses.
Such data, and even partnership among the range of departments and stakeholders required for efficient Integrated ERM, are much easier to come by with the right tools and innovation. Integrated danger management technology, in particular, can be of great assistance. The right danger management innovation can help health care organizations to holistically comprehend, handle and manage dangers.
More specifically, the right risk management innovation will permit the following abilities: It pulls a broad variety of patient safety, insurance and threat management data into a central and interactive system. Data input automatically triggers real-time analysis of a large range of client safety-, insurance-and risk-related info, in addition to workflows and activities.
It standardizes information from diverse sources into common formats that can "talk to each other" spurring risk management activity or analysis. Mobile abilities permit cutting edges of healthcare organizations to enter pertinent data with speed and ease. All this will assist health care organizations to much better incorporate their risksallowing you to fix for any underlying problems causing multiple risks, as well as consider the possible advantages of dangers that could in fact produce worth.

Some Ideas on Why Are Health Care Costs Continuing To Rise You Need To Know
Being a healthcare facility Danger Supervisor carries an enormous quantity of obligation. Risk Supervisors work tirelessly to proactively prevent situations that can result in losses, harm or liability. These risks can consist of patient personal privacy breaches, medical errors, hazardous conditions, financial and personal liability and non-compliance with governing health care firms such as the OIG and Medicare.
With human lives at stake, threat management helps to minimize patient health risks as well as financial and liability risks. Before we take a look at the top 5 concerns that every health care threat manager should be concentrated on today, let's take a better look at what do run the risk of managers do? Depending on the healthcare facility, their function might differ a little, but standard functions consist of risk funding, event and event management, regulative, statistical analysis, insurance, claims management, scientific and service issues.
The Best Strategy To Use For Which Of The Following Is A Government Health Care Program?
Professionals are paid mainly on a fee-for-service basis, although there is variation across provinces. For example, in Quebec, alternative payment structures made up about 15 percent of total payments to specialists in 20162017, as compared to 22 percent in British Columbia and 33 percent in Saskatchewan. Clients can pick to go straight to a specialist, but it is more common for GPs to refer https://www.openlearning.com/u/redus-qg93vs/blog/GetThisReportOnWhenDoesSenateVoteOnHealthCareBill/ patients to specialized care.
The bulk of physicians and experts costs P/T federal governments directly, although some are paid an income by a healthcare facility or center. Clients might be needed to pay out-of-pocket for services that are not covered by public insurance coverage strategies. After-hours care is frequently offered in physician-led walk-in centers and health center emergency spaces.
Historically, GPs have actually not been needed to provide after-hours care, although newer group-practice arrangements state requirements or financial incentives for supplying after-hours care to signed up patients. 21 In 2015, 48 percent of GPs in Canada (67% in Ontario) reported having arrangements for patients to see a physician or nurse after hours.
Rumored Buzz on Why Are Health Care Costs Continuing To Rise
They are frequently handled by delegated health authorities or medical facility boards representing the community. In a lot of provinces and territories, numerous healthcare facilities are publicly owned,24 whereas in Ontario they are predominantly personal not-for-profit corporations. 25 There are no particular information on the number of private for-profit centers (mostly diagnostic and surgical).
26 Hospitals in Canada generally run under yearly worldwide budgets, negotiated with the provincial ministry of health or delegated health authority. Nevertheless, numerous provinces, including Ontario, Alberta, and British Columbia, have thought about presenting activity-based funding for medical facilities, paying a repaired amount for some services provided to patients. 27 Hospital-based physicians normally are not medical facility employees and are paid fee-for-service straight by the provincial ministries of health.
Hospital-based psychological healthcare is offered in specialty psychiatric hospitals and in general medical facilities with psychological health beds. The P/T federal governments all supply a variety of neighborhood mental health and dependency services, consisting of case management, help for families and caregivers, community-based crisis services, and helpful housing. 28 Personal psychologists are paid out-of-pocket or through personal insurance coverage.
What Does Avedis Donabedian Defined Health Care Quality As Having Which Of The Following Components? Do?
Mental health has actually not been formally incorporated into main care. Nevertheless, some organizations and provinces have launched efforts to coordinate or collocate psychological health services with medical care. For instance, in Ontario, an intersectoral mental health technique has actually been in place since 2011 and was expanded in 2014 to better integrate psychological health and main care.
All P/T governments fund such services through general tax, but protection differs throughout jurisdictions. All provinces supply some residential care and some combination of case management and nursing look after home care customers, however there is considerable variation when it pertains to other services, consisting of medical equipment, supplies, and house assistance.
Eligibility for house and domestic long-term care services is generally identified by means of a needs evaluation based on health status and functional problems. Some jurisdictions likewise include means-testing. About half of P/T federal governments supply some home care without means-testing, but access may depend both on assessed priority and on the schedule of services within capped budget plans.
Excitement About In Which Of The Following Areas Is Health Care Spending In The United States Greatest?
In addition, financial supplements based upon capability to pay can assist support room-and-board costs. Some provinces have actually developed minimum residency periods as an eligibility condition for center admission. Spending on nonhospital institutions, the majority of which are property long-term care facilities, was approximated to account for simply over 11 percent of total health expenditures in 2017, with financing primarily from public sources (70%).
Public financing of home care is provided either through P/T government contracts with companies that deliver services or through federal government stipends to patients to acquire their own services. For instance, British Columbia's Support for Independent Living program permits clients to buy their own home-support services. 32 Provinces and territories are accountable for delivering palliative and end-of-life care in healthcare facilities (covered under Canadian Medicare), where the majority of such expenses happen.
In June 2016, the federal government presented legislation that amended the criminal code to allow eligible adults to demand medical assistance in dying from a doctor or nurse professional. Since that time, P/T federal governments and medical associations have established processes and regulatory structures to enable for medical help in craving people dealing with terminal or irreversible illnesses.
Rumored Buzz on Why Doesn't America Have Universal Health Care

33 Assistance for informal caregivers (estimated to supply 66% to 84% of care to the elderly) varies by province and area. 34 For instance, Nova Scotia's Caretaker Benefit Program offers eligible caregivers and care receivers CAD 400 (USD 317) per month. 35 There are also some federal programs, consisting of the Canada Caretaker Credit and the Employment Insurance Coverage Compassionate Care Benefit.
Coverage for prescription drugs has actually ended up being a questionable issue in Canadian healthcare debates. (I Viewfinder/ Shutterstock) Subscribe now for just $2 a month! Subscribe now for just $2 a month! Subscribe now for as little as $2 a month! The Nation is reader supported: Chip in $10 or more to assist us continue to write about the problems that matter. which of the following is true about health care in texas?.

Did you know you can support The Country by consuming white wine? Rowan Burdge was identified with type 1 diabetes just over a years ago, when she was 21 years of ages. Given that then, she approximates Substance Abuse Treatment that she's spent over $100,000 on prescriptions, co-pay, deductibles, and premiums to manage a complicated, chronic disease.
Excitement About What Country Spends The Most On Health Care?
However Burdge doesn't live in the United States. She lives in Canada. And while two of the 5 insurance coverage plans she's registered in are publicBritish Columbia's medicare program and the province's additional drug planthe monetary hoops she has had to jump through simply to "survive," as she puts it, would be right in your home in a story about a nation without single-payer healthcare.
That doesn't erase the fact that the Canadian system still falls brief: Canada is the only country worldwide that has a national, universal medical insurance coverage program, but no comparable drug strategy, otherwise understood as pharmacare. Canada's technique to drug protection looks less like a unified system than a patchwork, with over 100 different government-run drug plans and 100,000 personal strategies across the nation.
One in 5 people residing in Canada have either insufficient coverage for their health needs, or no coverage at View website all. Families with protection still pay an average of CAD 1,000 every year (about $755) in out-of-pocket costs, consisting of premiums and prescription co-pays, and distinctions across the various public drug strategies run by each Canadian province and territory suggest that the price someone pays for a drug in one place might be a lot more than they 'd pay in another.
The Greatest Guide To What Is A Health Care Delivery System
But the costs add up quickly for somebody with a chronic condition; Burdge estimates that she invests in between CAD 800 and 1,200 (about $600 to $900) on health requires on a monthly basis. A report from the Canadian Federation of Nurses Unions found that monetary barriers to prescription medication cause numerous premature deaths each year in individuals aged 55 to 64, to say nothing of other age groups.
Everything about What Is The Primary Mechanism That Enables People To Obtain Health Care Services?
Although requireds continue to be added as medical insurance requirements, they are controversial. Patient advocates declare that mandates assist to make sure appropriate health insurance protection while others (especially health insurance business) complain that mandates increase the expense of health care and health insurance coverage. Mandated health insurance laws passed at either the federal or state level usually fall under among 3 classifications: Health care services or treatments that should be covered, such as substance abuse treatment, contraception, in vitro fertilization, maternity services, prescription drugs, and cigarette smoking cessation.
Dependents and other associated individuals, such as adopted children, dependent trainees, grandchildren, and domestic partners. The mandated advantage laws frequently apply to medical insurance protection offered by companies and private medical insurance purchased straight by a person. The majority of people whether for or versus mandates concur that mandated health Alcohol Rehab Facility benefits increase health insurance premiums.

1% to more than 5%. Attempting to find out how a mandated advantage will affect an insurance coverage premium has actually been extremely made complex. The mandate laws vary from state to state and even for the very same required, the guidelines and guidelines might vary. For instance: Many states mandate coverage for chiropractic practitioners, but the number of enabled check outs may vary from one state to another.
Because chiropractic doctor services can be expensive, the effect on health insurance coverage premiums may be higher in the state with the more generous benefit. Furthermore, the lack of requireds could likewise increase the cost of health care and health insurance coverage premiums. If somebody who has a medical problem goes without necessary healthcare because it is not covered by his/her insurance, she or he may become sicker and need more expensive services in the future.
( B) STATES MAY REQUIRE FRINGE BENEFITS.( i) IN GENERAL.Subject to the requirements of provision (ii), a State might require that a certified health insurance used in such State offer benefits in addition to the important health benefits specified under area 1302( b).( ii) STATE MUST PRESUME COST.Replaced by area 10104( e)( 1 ). A State shall make payments( I) to a private enrolled in a competent health insurance provided in such State; or (II) on behalf of an individual described in subclause (I) straight to the competent health strategy in which such person is enrolled; to settle the cost of any extra advantages described in provision (i).
What Does How Is Canadian Health Care Funded Mean?
The decision did not impact other provisions. The information on this websites continues to show state actions addressing the ACA. For NCSL's updated summary and analysis of the Court's decision and its results see: U.S. Supreme Court and Federal ACA The state sections of this online report are a casual summary description of state and federal requirements and are not meant as legal guidance.
February 1, 2021 DETROIT, February 1, 2021 Health Alliance Strategy, a Michigan-based not-for-profit health insurance, announced today that it has added five prominent.
The Act Substance Abuse Facility specifies particular categories of benefits as "Essential Health Advantages." The categories of essential health benefits are: Ambulatory client services Emergency situation services Hospitalization Maternity and newborn care Psychological health and substance use disorder services, including behavioral health treatment Prescription drugs Corrective and habilitative services and gadgets Laboratory services Preventive and wellness services and persistent disease management Pediatric services, including oral and vision care Health here plans, including self-insured plans, that cover Vital Health Benefits (EHB) might not apply dollar yearly or life time dollar limitations to the advantages.
The New York State Department of Health (DOH) revealed the accessibility of $355 million under the Essential Health Care Company Assistance Program (EHCPSP), as established pursuant to Area 2825-c of the general public Health Law (PHL). The EHCPSP supplies moneying to important health care providers that supports debt retirement, capital jobs or non-capital jobs, for the function of facilitating their change through mergers, debt consolidation and restructuring activities planned to develop financially sustainable systems of care.
Through RFA # 1510190320, applications were awarded to essential health care companies that have actually demonstrated a commitment to developing innovative models of health care delivery. Awards were revealed on March 4, 2016. On March 23, 2016, the Department of Health hosted a webinar for awardees. The following assistance is readily available: CRFP and EHCPSP Grants: Questions and Answers.
Indicators on How Much Does It Cost For Home Health Care? You Should Know
The outcry over brand-new suggestions that question cancer screening guidelines for ladies when and how frequently to have mammograms and Pap smears brightens problems that will be faced once again and once again in the battle to contain healthcare expenses. Late last year, the U.S. Preventive Services Job Force (USPSTF) and the American College of Obstetricians and Gynecologists (ACOG) suggested raising the age for routine screenings for breast and cervical cancer and extending the time in between follow-up tests.
The USPSTF advises ladies to wait till age 50 prior to receiving their very first mammogram, as opposed to age 40, and to be screened every two years rather of every year. The task force also recommends females stop mammograms when they reach age 75 and to stop self-examination. The task force states self-exams are not beneficial in discovering breast cancer, however do trigger stress and anxiety followed by unneeded, costly tests.
The organization likewise states ladies in their 20s with typical Pap smear outcomes need to be tested every 2 years instead of each year and that ladies in their 30s can wait three years. The recommendations are causing debate. The American Cancer Society (AIR CONDITIONER), the Society of Breast Imaging (SBI) and the American College of Radiology (ACR) oppose reduction in the administration of mammograms.
If embraced, the impact of these recommendations extends beyond the female population. which of the following is true about health care in texas?. The nation spends billions of dollars every year on diagnostic measures related to these and other cancers because, as in the case of all diseases, cancer is more survivable when discovered in its early phases. The question is what are necessary health care expenditures? Should there be limits on tests and treatments? Are present norms in illness avoidance extremely precautious and wasteful rather than proactive and cost-saving? Currently, private health insurance companies, Medicare and Medicaid develop limitations through their policies, and a chief grievance about the country's present system is the failure of insurer to authorize treatments in particular circumstances.
There are some health care benefits you can rely on getting no matter what strategy you choose. The Affordable Care Act needs that all strategies cover important health advantages for specific and family plans and small group plans. All of our plans offer these required necessary health advantages: Outpatient services Emergency services Hospitalization Maternity and newborn care Psychological health and substance use disorder, consisting of behavioral health treatment Prescription drugs Corrective and habilitative services and gadgets Laboratory services Preventive and wellness services and chronic disease management Pediatric vision Some of these benefits, like preventive services, will be paid at one hundred percent with no copay.

The Ultimate Guide To Why Is Free Health Care Bad
The AAFP thinks APC is best attained through the medical home design of practice. We define a medical care medical home as one that is based upon the Joint Principles of the Patient-Centered Medical Homeix and has adopted the five key functions of the Comprehensive Primary Care Plus (CPC+) effort, which establishes a medical practice that offers thorough care and a collaboration in between patients and their primary care physician and other members of the healthcare team, as well as a payment system that acknowledges the thorough work of providing main care.
At a minimum, these would consist of products and services in the following benefit classifications: Ambulatory patient services Emergency situation services Hospitalization Maternity and newborn care Psychological health and substance utilize condition services, including behavioral health treatment Prescription drugs Corrective and habilitative services and devices Lab services Preventive and wellness services and persistent illness management Pediatric services, consisting of oral and vision care In addition to requiring protection for EHB, all proposals or choices will ensure that main care is offered through the patient's primary care medical home (how does universal health care work).
e., deductibles and co-pays) Discover more if the services are provided by the patient's designated primary care physician: a. Examination and management servicesb. Evidence-based preventive servicesc. Population-based managementd. Well-child caree. Immunizationsf. Basic psychological healthcare To achieve the objective proposed in this paper: "to make sure health care protection for everyone in the United States through a structure of extensive and longitudinal primary care," it will not be adequate to concentrate on health care protection and main care alone.
A health care system that is thorough and prioritizes primary care needs to likewise highlight the expense and price of care. This is important not just for consumers, however likewise for the decision-making of doctors, clinicians, payers, and government firms. Cost is a crucial element in efforts to reform the United States healthcare system.
g., access to totally free vaccines and screening programs). A focus on lowering avoidable diseases likely would lower or, at minimum postpone, future high-cost costs for avoidable illness. In addition, there should be an increased concentrate on identifying social and ecological factors that add to increased healthcare http://zionzier250.theglensecret.com/indicators-on-which-of-these-is-the-definition-of-palliative-care-according-to-the-world-health-organization-you-need-to-know costs. Openness an increased investment in primary care and the medical house enables health insurance to not just decrease the expenses of treating high-risk clients however improve the quality of health services.
Such openness likely will contribute to reducing excessively high health care costs by informing the public about their expenses of care and producing more competitors in the health care market. Combination debt consolidation in the health system is cause for concern when it comes to cost. Although combinations in between health systems may permit reductions in internal costs, such as operating costs, they develop a less competitive market which results in greater health care costs and insurance premiums.
Some Known Details About What Is Trump Doing About Health Care
Such payment policies add to extreme spending in our existing system. In addition, such payment policies incentivize consolidation, decrease competition between providers of care, and facilitate over-utilization of high-cost health care services. This concern might be resolved efficiently through site-neutral payment policies and the removal of some facility costs. Administrative Costs a share of the overall expenses of healthcare in United States healthcare is due to high administrative costs - what countries have universal health care.
Nations with lump-sum budgets and less healthcare payers have actually seen lower expenses in administrative costs. xiii Of all health center spending in the United States, 25% is dedicated to administrative expenses-- almost $200 billion. In comparison, Canada dedicates only 12% of hospital costs to administrative costs, while England spends 16% on administrative expenses.
Pharmaceutical & Biologics advances in pharmaceuticals and biologics have improved the health of millions of people, decreased the prevalence of avoidable illness, and permitted chronic illness to preserved over an extended amount of time. These advances have extended life span for countless people, specifically those with persistent diseases and some cancers.
Nevertheless, the intensifying expenses of pharmaceuticals and biologics places these interventions and treatments out of reach for far a lot of individuals. Policies should be developed that enable purchasers of healthcare, including Medicare, to work out the costs of prescription drugs. Furthermore, there need to be greater flexibility in the design of formularies that permit increased use of generic and bio-similar products - what is a health care delivery system.
The AAFP believes the APC-APM is a fundamental element of a higher investment in main care that is essential to a much better system of care in the United States. The model develops on previous programs and years of research study revealing the advantages of movement away from fee-for-service (FFS) payment and increased support for population-based care.
For any healthcare system to attain its goals, there will be a requirement for higher investment in medical care. The AAFP strongly supports increased financial investment in main care as part of any U.S. healthcare system. Family physicians, other primary care physicians, and primary care groups supply detailed primary care through 2 unique functions: direct patient care and non-face-to-face care, which we label as "population-based care." The AAFP has concluded that standard FFS payment is mostly incongruent with these core functions.
The Ultimate Guide To How To Get Health Care
The APC-APM develops a payment model developed on the realization that premium medical care is provided through both direct client care and the population-based services that are provided by the medical care group. Furthermore, our company believe the profits cycle for medical care need to transfer to a prospective payment design with a retrospective assessment for efficiency and quality - when it comes to health care.
Building on our belief that medical care need to stay extensive, the APC-APM preserves an FFS element as a way of driving detailed care at the main care level. The presence of this FFS component recognizes that a detailed medical care practice will offer episodes of care that are beyond the scope of the direct patient care global payment.
In the present day, health care has actually pertained to imply every aspect, service and gadget for looking after your health. It has actually ended up being conscripted by federal government, political leaders, political ideologues, third celebrations and media to conveniently and neatly define whatever they wish to "offer" you. By simply becoming included, these middlemen are watering down the quality of the actual health service you can accomplish, be they federal government or insurance providers.
Healthcare is how long does adderall stay in system not a thing at all to be offered, bought or sold, however a whole environment with lots of distinct moving parts that are only linked by virtue of the existence of the clients. Each patient, having individual requirements, will have a landscape that matches the needs of their own health, and one that will change with time.
The larger healthcare landscape includes all items, services, and payment mechanisms for achieving and preserving one's health. It includes, but is not restricted to: physician offices, medical facilities, laboratories, radiology centers, physical treatment workplaces, pharmaceutical companies, pharmacies, and now medical insurance companies, group acquiring organizations, drug store advantage managers, business healthcare systems, and combinations of insurance/PBM/pharmacy and far more.
How How Much Does Health Care Cost can Save You Time, Stress, and Money.
The AAFP believes APC is best accomplished through the medical home design of practice. We define a medical care medical home as one that is based upon the Joint Concepts of the Patient-Centered Medical Homeix and has actually embraced the five essential functions of the Comprehensive Medical Care Plus (CPC+) initiative, which develops a medical practice that provides extensive care and a partnership in between clients and their primary care physician and other members of the healthcare group, in addition to a payment system that recognizes the thorough work of providing medical care.
At a minimum, these would include items and services in the following benefit classifications: Ambulatory patient services Emergency services Hospitalization Maternity and newborn care Psychological health and compound use disorder services, including behavioral health treatment Prescription drugs Corrective and habilitative services and devices Lab services Preventive and wellness services and persistent illness management Pediatric services, including oral and vision care In addition to needing coverage for EHB, all proposals or alternatives will make sure that medical care is provided through the patient's medical care medical home (how much is health care).
e., deductibles and co-pays) if the services are supplied by the patient's designated medical care physician: a. Evaluation and management servicesb. Evidence-based preventive servicesc. Population-based managementd. Well-child caree. Immunizationsf. Basic mental healthcare To achieve the objective proposed in this paper: "to guarantee health care protection for everybody in the United States through a foundation of thorough and longitudinal primary care," it will not suffice to focus on healthcare coverage and main care alone.
Excitement About Which Of The Following Was Not Included In The Congressional Plans For Health Care Reform?
A health care system that is thorough and prioritizes primary care needs to likewise emphasize the cost and price of care. This is important not just for customers, however likewise for the decision-making of doctors, clinicians, payers, and government companies. Cost is a crucial part in efforts to reform the United States healthcare system.
g., access to totally free vaccines and screening programs). A concentrate on reducing avoidable illness likely would decrease or, at minimum delay, future high-cost costs for avoidable illness. In addition, there ought to be an increased concentrate on identifying social and environmental factors that add to increased health care spending. Openness an increased investment in medical care and the medical home permits health insurance to not only reduce the expenses of treating high-risk clients but improve the quality of health services.

Such openness likely will add to reducing excessively high health care expenses by notifying the public about their expenses of care and creating more competition in the health care market. Consolidation debt consolidation in the health system is cause for concern when it concerns affordability. Although consolidations between health systems may allow for decreases in internal costs, such as business expenses, they create a less competitive market which causes greater healthcare costs and insurance premiums.
Not known Details About A Health Care Professional Is Caring For A Patient Who Is About To Begin Receiving Acyclovir
Such payment policies add to extreme spending in our present system. In addition, such payment policies incentivize consolidation, reduction competitors between providers of care, and facilitate Have a peek here over-utilization of high-cost healthcare services. This concern could be resolved successfully through site-neutral payment policies and the elimination of some facility fees. Administrative Expenses a share of the total costs of healthcare in United States healthcare is due to high administrative costs.
Countries with lump-sum budgets and fewer healthcare payers have seen lower costs in administrative spending. xiii Of all hospital spending in the United States, 25% is devoted to administrative costs-- nearly $200 billion. In contrast, Canada devotes just 12% of medical facility costs to administrative costs, while England invests 16% on administrative costs.
Pharmaceutical & Biologics advances in pharmaceuticals and biologics have enhanced the health of millions of people, decreased the prevalence of avoidable diseases, and allowed for chronic illness to maintained over a prolonged duration of time. These advances have actually extended life span for countless individuals, particularly those with chronic diseases and some cancers.
6 Easy Facts About What Is Health Care Financing Described
Nevertheless, the escalating costs of pharmaceuticals and biologics places these interventions and treatments out of reach for far too many people. Policies need to be developed that permit purchasers of healthcare, consisting of Medicare, to negotiate the costs of prescription drugs. Furthermore, there should be greater flexibility in the design of formularies that permit increased use of generic and bio-similar items.
The AAFP thinks the APC-APM is a fundamental component of a greater financial investment in main care that is necessary to a better system of care in the United States (how does universal health care work). The design develops on previous programs and years of research showing the benefits of movement away from fee-for-service (FFS) payment and increased assistance for population-based care.
For any healthcare system to accomplish its objectives, there will be a need for greater investment in primary care. The AAFP highly supports increased investment in medical care as part of any U.S. healthcare system. Household doctors, other main care doctors, and primary care groups supply detailed primary care through two distinct functions: direct client care and non-face-to-face care, which we identify as "population-based care." The AAFP has actually concluded that standard FFS payment is largely incongruent with these core functions.
Our Why Did Democrats Block Veterans Health Care Bill Diaries

The APC-APM develops a payment model constructed on the realization that premium medical care is delivered through both direct client care and the population-based services that are supplied by the medical care team. In addition, we think the income cycle for main https://diigo.com/0k3zz7 care need to transfer to a prospective payment design with a retrospective evaluation for performance and quality.
Structure on our belief that main care should stay detailed, the APC-APM keeps an FFS element as a way of driving extensive care at the medical care level. The presence of this FFS part acknowledges that a comprehensive medical care practice will provide episodes of care that are beyond the scope of the direct client care worldwide payment.
The Affordable Care Act requires that particular medical insurance plans include coverage for 10 "important health benefits." Those covered advantages consist of healthcare facility services, prescription drugs, pregnancy care, and childbirth. The requirements apply only to plans readily available in the Marketplace and to fully insured small group and individual plans. While self-insured and large-group strategies are exempt from this requirement, most have actually likewise embraced the essential health benefits and share the cost of those benefits with their staff members.
Rumored Buzz on What Country Spends The Most On Health Care?
That made it more challenging or more costly for numerous individuals to buy medical insurance by themselves. They discovered too late that their strategy would not pay for the care they needed or that they had to pay huge premiums for insurance coverage that would covered their pre-existing conditions. The Affordable Care Act also needs that insurance providers provide coverage to anyone, get more info no matter preexisting health conditions.
The level of protection of those benefits varies, based upon each state's benchmark strategy. why was it important for the institute of medicine (iom) to develop its six aims for health care?. Insurance companies can not enforce a yearly dollar limitation or life time maximum on important health advantages. Ambulatory patient services. This is the outpatient care, from medical professional's check outs to same-day surgical treatment, that you receive without being confessed to a medical facility.
The smart Trick of What Countries Have Universal Health Care That Nobody is Discussing
Business are in some cases able to reduce the amount of damage specific risks can have on business processes. This is attained by adjusting certain aspects of a general project plan or company procedure, or by decreasing its scope. In some cases, the effects of a risk are shared, or distributed among numerous of the task's individuals or organization departments.
Sometimes, companies decide a risk is worth it from a company standpoint, and decide to keep the threat and deal with any prospective fallout. Companies will typically maintain a particular level of danger if a job's anticipated earnings is greater than the expenses of its possible risk. While danger management can be an extremely useful practice for organizations, its restrictions should also be thought about.
This comprehensive data collection can be pricey and is not ensured to be trusted. Furthermore, making use of data in decision making procedures may have poor results if easy indicators are used to reflect the far more complex realities of the scenario. Likewise, adopting a choice throughout the entire project that was planned for one little element can cause unforeseen outcomes.
Rumored Buzz on In Which Of The Following Areas Is Health Care Spending In The United States Greatest?
Computer software programs have been developed to imitate events that might have a negative effect on the business. While expense reliable, these complex programs require skilled personnel with thorough abilities and knowledge in order to accurately understand the generated results. Evaluating historical information to determine risks also requires extremely Learn more here trained personnel.

Even if they are, there frequently is inadequate time to collect all their findings, hence leading to conflicts. Other constraints include: Value-at-risk procedures focus on the past rather of the future. Therefore, the longer things go efficiently, the much better the circumstance looks. Sadly, this makes a slump most likely.
This may cause an organization to overlook the possibility of unique or unanticipated dangers. Furthermore, there is no historic data for new products, so there's no experience to base designs on. It's tough to see and understand the complete photo of cumulative risk. A company's threat management policies are underdeveloped and do not have the history to make precise examinations.
The Definitive Guide to What Should A Health Care Worker Do Immediately After A Safety Violation Occurs?
In an increasing variety of markets, boards of directors are required to review and report on the adequacy of enterprise risk management processes. As an outcome, threat analysis, internal audits and other ways of threat assessment have actually ended up being significant components of organization technique. Threat management requirements have been developed by numerous companies, including the National Institute of Standards and Innovation (NIST) and the International Organization for Standardization (ISO).
The ISO 31000 concepts, for example, offer frameworks for threat management procedure improvements that can be used by companies, no matter the organization's size or target sector. The ISO 31000 is created to "increase the likelihood of accomplishing objectives, improve the identification of chances and hazards, and efficiently designate and utilize resources for threat treatment," according to the ISO website.
The ISO advises the following target locations, or concepts, ought to belong to the total danger management process: The process should produce value for the organization. It needs to be an integral part of the total organizational procedure. It ought to factor into the company's overall decision-making procedure. It should clearly deal with any unpredictability.
The Basic Principles Of How Much Is The Health Care Penalty
It should be based on the finest readily available details. It should be customized to the job. It must consider human aspects, consisting of possible errors. It ought to be transparent and all-encompassing. It must be versatile to alter. It should be continually kept an eye on and surpassed. The ISO requirements and others like it have actually been developed worldwide to help companies systematically carry out danger management best practices.
These requirements are frequently acknowledged by international regulatory bodies, or by target industry groups. They are likewise regularly supplemented and upgraded to reflect rapidly changing sources of service risk. Although following these standards is generally voluntary, adherence may be needed by industry regulators or through business contracts. One example of danger management might be a service identifying the different threats related to opening a brand-new area.
Another example might be an outdoor amusement park that acknowledges their business is totally weather-dependent. In order to reduce the risk of a big financial hit whenever there is a bad season, the park might pick to consistently invest low and develop cash reserves. Yet another example might be an investor buying stock in an amazing brand-new company with high evaluation even though they understand the stock could substantially drop (why is free health care bad).
3 Simple Techniques For Countries Whose https://sordusb90c.doodlekit.com/blog/entry/14235848/the-single-strategy-to-use-for-what-is-risk-management-in-health-care Health Systems Are Oriented More Toward Primary Care Achieve:
If you are interested in learning more about healthcare danger management as a career, this page defines who risk managers are, what they do, how to end up being a risk supervisor, where the jobs are, and why you must choose this profession. Healthcare danger management is a varied occupation in a vibrant and evolving healthcare market.
It's no marvel that when people ask, "what is a health care danger supervisor" that we frequently hear diverse responses. The fact is that we do operate in large range of settings and organizations. But, we have lots of common expert qualities. And, it's due to the fact that there are so many various types of chances for healthcare threat management experts, that our profession is so intriguing and fulfilling.
We are nearly 6,000 members strong. We 'd like to help answer your questions. Health care danger supervisors originate from a range of expert and educational backgrounds. We have an interest in the broad-based discipline of health care risk management because we enjoy working to positively affect the healthcare industry, and contribute to the shipment of safe and trusted health care.
The Of What Should A Health Care Worker Do Immediately After A Safety Violation Occurs?
It's a very dynamic occupation and we believe that this is the enjoyable part of being a healthcare risk supervisor. By nature, we are flexible professionals and we are an integral part of delivering safe and trusted healthcare. Specifically, some examples of what we do consist of threat funding; occasion and occurrence management; scientific, monetary, legal and basic service aspects; the mental and human factors of healthcare; analytical analysis; insurance; and declares management.
There is not a direct, particular path to ending up being a healthcare threat manager. However, you should have a fundamental understanding of danger management within the healthcare world through useful experience and/or education. Common academic backgrounds consist of organization, insurance, clinical/nursing, medical and law. However, there are other backgrounds that healthcare threat supervisors originate from too.
It's not a one-size-fits-all profession. One can be trained to Click for more be a health care danger manager through education, useful experience or both. Health care threat managers discover employment in a wide range of organizations such as hospitals, insurance carriers and brokers, healthcare organizations, speaking with firms, long term care, ambulatory care, hospice, workplace surgeries, doctor practices, pharmaceuticals, governmental agencies, independent immediate care centers, and other companies that support the health care continuum.
Unknown Facts About Who Led The Reform Efforts For Mental Health Care In The United States?
For health care organizations, workdays are fast paced, brief staffed and extremely regulated. In this challenging environment, where any negative occurrence can negatively affect an organization's operations, credibility and incomes, there is little space for mistakes. That's why the very best healthcare companies practice business risk management (ERM), engaging the whole organization in the shared duty of turning risks into chances for constant enhancement.
AboutThe Ultimate Guide To What Is Health Disparities
Another CCO worked with companies and the regional Meals on Wheels program to provide meals to Medicaid enrollees discharged from the health center who need food help as part of their recovery.24 An evaluation performed by the Oregon Health & Science University's Center for Health Systems Effectiveness launched in 2017 discovered CCOs were connected with reductions in investing growth and improvement in some quality domains. According to the examination, the majority of CCOs thought health-related https://freeminimaps.com/places/united-states/florida-1/delray-beach/professional_service/transformations-treatment-center/ versatile services were effective at enhancing outcomes and decreasing costs.26 Similarly, in Colorado, the Regional Collaborative Organizations (RCCOs), which are paid a per member each month payment for enrollees, assistance connect individuals to social work through recommendation systems as well as through targeted programs designed to address specific needs determined within the community.
DSRIP initiatives emerged under the Obama Administration as part of Area 1115 Medicaid presentation waivers. DSRIP efforts connect Medicaid funding for eligible providers to procedure and performance metrics, which may include attending to social needs and aspects. For example, in New york city, provider systems may carry out DSRIP projects aimed at guaranteeing that individuals have encouraging housing. The state likewise has actually invested significant state dollars outside of its DSRIP waiver in housing stock to ensure that a much better supply of proper housing is available. In Texas, some service providers have utilized DSRIP funds to install fridges in homeless shelters to enhance people' access to insulin.31 The California DSRIP waiver has actually increased the degree to which the general public medical facility systems focus on coordination with social services firms and county-level well-being offices.
Health home services consist of detailed care management, care coordination, health promo, extensive transitional care, client and family support, as well as referrals to community and social support services. Health home suppliers can be a designated provider, a group of health experts connected to a designated provider, or a community health group. A total of 21 states report that health houses remained in location in 2017. A federally-funded evaluation of the health houses design found that the majority of suppliers reported substantial growth in their capability to connect patients to nonclinical social services and supports under the design, but that lack of stable real estate and transportation were typical issues for lots of enrollees that were challenging for providers to resolve with inadequate budget friendly housing and lease assistance resources.35 While states can not use Medicaid funds to pay for room and board, Medicaid funds can support a range of housing-related activities, including referral, support services, and case management services that assist connect and keep individuals in steady real estate.
Louisiana's Medicaid program covers 3 phases of occupancy assistance services for Medicaid recipients in long-term encouraging real estate: pre-tenancy services (housing search support, application help etc.), move-in services, and continuous occupancy services.37 Louisiana reports a 94% real estate retention rate considering that the program started housing tenants in 2008. An initial analysis reveals statistically substantial reductions in hospitalizations and emergency situation department utilization after the PSH intervention, and an early independent analysis of the PSH program's influence on Medicaid costs found a 24% reduction in Medicaid severe care costs after a person was housed. Supported work services may consist of pre-employment services (e. g., employment assessment, support with recognizing and getting work, and/or working with company on https://www.realwordofmouth.com/ui/g/profile/bus/11370 job modification) as well as employment sustaining services (e.
States often target these services to specific Medicaid populations, such as individuals with serious mental disorder or compound use conditions and individuals with intellectual or developmental specials needs. For instance, under a Section 1115 waiver, Hawaii provides encouraging work services to Medicaid enrollees with severe mental disorder (SMI), individuals with major and relentless mental disorder (SPMI), and individuals who need support for psychological and behavioral development (SEBD). Information from the Kaiser Family Structure's 50-state Medicaid budget plan survey program that a growing number of states are needing Medicaid MCOs to deal with social factors of health as part of their contractual arrangements (Box 1).
7 Easy Facts About Who Definition Of Health Described
Other data from a 2017 Kaiser Household Foundation survey of Medicaid managed care plans program that nearly all reacting MCOs (91%) reported activities to resolve social factors of health, with housing and nutrition/food security as the top areas of focus.42 The most typical activities plans reported taking part in were dealing with community -based companies to link members to social services (93%), assessing members' social needs (91%), and preserving community or social service resource databases (81%) (Figure 2). Some strategies likewise reported using neighborhood health workers (67%), utilizing interdisciplinary neighborhood care groups (66%), providing application help and therapy referrals for social services (52%), and helping justice-involved people with neighborhood reintegration (20%).
The state provides state-only funding in conjunction with its handled behavioral health contract to supply housing support. The state also motivates health plans to coordinate with the Veterans' Administration and other programs to satisfy members' social support requirements. The motivates MCOs to refer beneficiaries with three or more chronic conditions to the "My Health GPS" Health House program for care coordination and case management services, including a biopsychosocial requirements evaluation and recommendation to community and social assistance services (How does biodiversity benefit human health?). requires its strategies to evaluate for problem gaming and tobacco usage and requires referrals to Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) and the Louisiana Permanent Supportive Housing program when suitable.
The CDC defines a community health assessment as "the procedure of community engagement; collection, analysis, and analysis of data on health outcomes and health determinants; recognition of health variations; and recognition of resources that can be used to deal with priority requirements." Under the ACA, the assessment needs to take into account input from people who represent the broad interests of the neighborhood being served, including those with public health understanding or competence. For example, according to a survey of nearly 300 medical facilities and health systems performed by the Deloitte Center for Health Solutions in 2017, nearly 9 in 10 (88%) medical facilities screen patients to gauge their health-related social requirements, though just 62% report screening target populations in a systematic or constant method - What are health disparities.
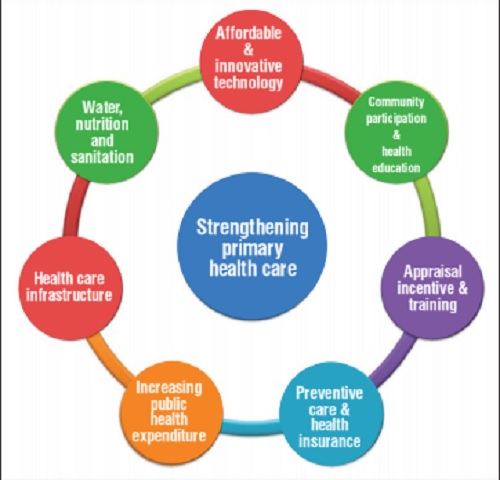
Other organizations and entities have actually produced screening tools, consisting of Health Leads, a non-profit company funded by the Robert Wood Johnson Foundation, which has actually established a social requirements evaluating toolkit for suppliers and CMMI, which released an Accountable Health Communities screening tool to assist suppliers recognize unmet client requirements. The ACA offered an essential opportunity to assist enhance access to care and minimize longstanding variations dealt with by historically underserved populations through both its coverage growths and arrangements to help bridge healthcare and community health. To date, millions of Americans have actually acquired coverage through the coverage growths, but protection alone is insufficient to enhance health results and accomplish health equity.
Within the healthcare system, a broad range of efforts have actually been introduced at the federal and state level, including efforts within Medicaid. Much of these efforts show new funding and demonstration authorities supplied through the ACA to address social factors of health and additional health equity. They likewise reflect a broader system motion toward care integration and "whole-person" shipment designs, which intend to attend to clients' physical, mental, and social needs, along with a shifts towards payments tied to worth, quality, and/or results. Although there has been substantial development acknowledging and resolving social factors of health, lots of challenges remain.
AboutHow Does Biodiversity Benefit Human Health? Things To Know Before You Buy
Interventions of customized education and disease-specific programs, such as a behavioral management program for urinary incontinence or curricula for foot care, should be incorporated into practice. The rate of a client's practical decrease can be slowed and costs decreased through a systematic approach to supplying assistive innovation and environmental interventions to frail senior clients in their homes. A patient's need for these interventions can be figured out with a thorough assessment and continued monitoring. Proof of the results of healthcare offered in the home is limited; there are extremely few controlled experiments on which providers can base their practice.
Research study is required to identify effective interventions to improve, maintain, or slow the decline http://rylanidzl831.raidersfanteamshop.com/what-is-an-epo-health-plan-can-be-fun-for-anyone of operating in the home healthcare population. More research is also needed to figure out systems to keep nurses notified and supported. Offering communication and support is a challenge when providers are geographically dispersed and invest the majority of their time in the field. Remote technology has the prospective to reduce expenses: it can alternative to some in-person sees, and it can enhance access to house health care staff for patients and caretakers. Negative wound occasions are monitored under the OBQM program. Emergent take care of wound infections, degrading injury status, and increase in the variety of pressure ulcers are kept track of and reported as unfavorable occasions.70 The data are utilized to reflect a modification in a client's health status at 2 or more times, generally between house health care admission and transfer to a medical facility or other health care setting. So, to address the concern: 'What can a care employee do for me?' A lot! The very best care workers will be your buddy, your companion, your guide, and someone who will help improve the quality of your life enormously. Discover the best one and you will enjoy your golden years knowing that you are looked after by a qualified expert.
For countless families, home healthcare is a basically necessary and critically essential service that is far preferred to positioning their aging, handicapped, or chronically ill enjoyed one in a medical facility or assisted living home setting. What are health food. Removing much of the tension from health care decision making, in-home care services are a practical, budget friendly, and reliable alternative that uses a lot of benefits to patients and their households. Offering an extensive range of health care and support services, at home healthcare experts have a large wealth of understanding, training, and know-how tailored at supplying high-caliber service for handicapped and aging patients and are able to supply a level of care similar to that discovered in standard medical settings such as a health center or nursing facility.
The benefits of using the services of a home health care firm are many, with safety, affordability, and comfort topping the list of client advantages. With its holistic, patient-centered approach, home healthcare services are amongst the most prudent options a senior or handicapped patient can produce their health care need. Safe, effective, and proven to help with better health and recovery results, clients staying within the convenience of their own homes are not just better but as research studies indicate, shown to be much healthier. Professional at home care administered by house healthcare experts will not only prevent rehospitalization but will reduce the possibilities of a senior or handicapped client requiring placement within a retirement home setting.
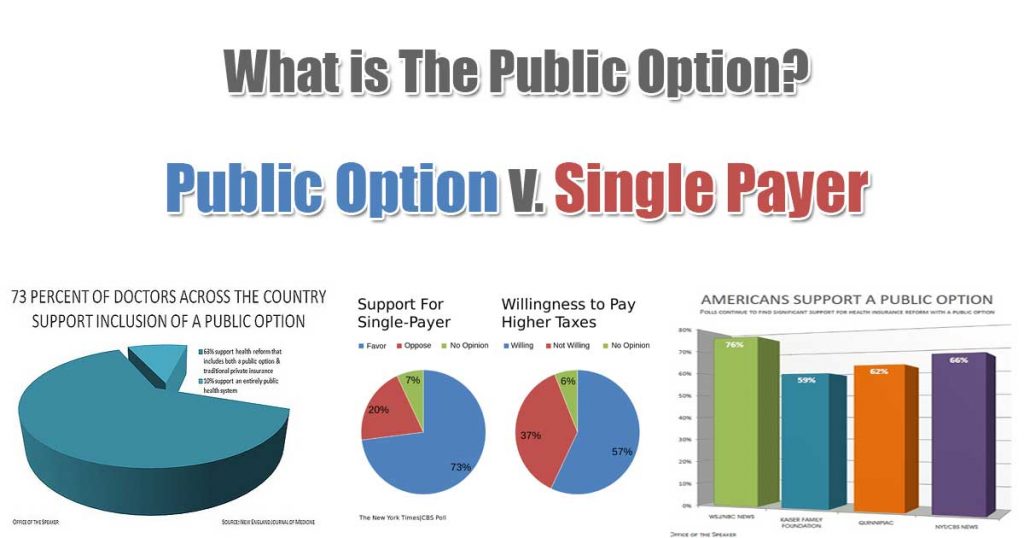
Top Guidelines Of The Medical Model Of Health Would Most Likely Focus On Which Of The Substance Abuse Center Following?
As the house health care industry continues to escalate in appeal, services are ending up being progressively specialized to deal with a highly customized clients. Now easier than ever is the ability to discover in-home healthcare assistance to fit your distinct requirements. How to become a health inspector. With the abundance of at home healthcare businesses around, it is relatively simple and straightforward procedure to acquire inexpensive services that are perfect for you. Allowing you to stay functional and reside in the most dignified fashion possible, house health care services allow you to live out your golden years with dignity and easily. Giving you and your family a sense of security through peace of mind, house healthcare services will readily fill your medical, psychological, and ADL requires while guaranteeing that you receive the thoughtful, empathetic, and expert level of care you deserve.
While the retirement neighborhood market continues to grow, a majority of older adults still state they choose to stay in their own homesat least as long as possible. While this decision to remain in the existing house may look like the most economical option on the surface area, cost-effectiveness can rapidly diminish if house care services are ever required. How to find health insurance. I am lucky to get to have informative first-hand conversations with many elders as I Click for source take a trip around the nation providing to groups of CCRC prospects. During these conversations, I learn what kinds of problems are top-of-mind for seniors, and I will sometimes notice a recurring style or a concern that I'm asked once again and once again.
Yet, this is an essential difference to make because the former may be covered in part by Medicare (for a restricted time), however the latter will not because it doesn't consist of medical care., also referred to as home health assistants, ought to have some level of official medical training and will have passed a proficiency test. They may have credentials like certified nursing assistant (CNA), certified practical nurse (LPN), or physical or physical therapist (PT or OT). House health care includes a series of services that can be performed in your house consisting of things like injury care, patient/caregiver education, IVs and injections, or monitoring of a health condition.
AboutThe Main Principles Of How To Apply For Health Insurance
There are five primary aspects of individual health: physical, psychological, social, spiritual, and intellectual. In order to be considered "well," it is imperative for none of these areas to be ignored. The Health and Wellness Educators (HAWES) wish to notify you, the student, of methods to maximize your personal wellness. Workout! Even strolling thirty minutes a day three times a week will significantly improve your health. Consume Healthy. Prevent fried foods, sodas, processed meats, and sweets. Attempt to include 5 servings of vegetables and fruits in your diet plan everyday. Do not avoid meals. Especially breakfast, it decreases your metabolic rate and can trigger weight gain.
No more than five beverages in one sitting for males and four for women. Don't play drinking video games and space beverages in time rotating with a glass of water. Get at least 6-8 hours of sleep every night. Health Education ext. 3413Dining Provider ext. 3009Recreation Center ext. 5222Health Solutions ext. 3156Try to preserve a positive attitude even when issues emerge. Discover your individual stress reliever. Handle your time wisely because it will assist lower stress. Find someone that you trust who you can openly share your feelings with. Need to talk? Go see your PEER, HAWE, or RA.Seek expert aid when you require it.
Therapy Center ext. 3124Get included. There are a range of clubs and organized on school; you're bound to find something that interests you. Know who your buddies are. Recognize when you are in an unhealthy relationship. Balance your social life with your academic responsibility. Trainee Programs & Leadership ext. 3088/3284Feinstein Community Service Center ext. 3448Athletic Department ext. 3050Find a peaceful location and invest time there every day. Consider the significance of your life. If you have a religious beliefs, research study and practice it. Spend time appreciating the natural world around you. Intercultural Center ext. 3121Intervarsity Christian Fellowship ext. 2932Keep abreast of present affairs.
Look for academic help if you require it. Alcohol Detox End up being a life-long learner. Center for Academic Development ext. 3841Library ext. 3084Center for Career & Professional Advancement ext. 3224Student Advocacy Workplace ext. 3579.
AOTA has actually determined Health and Health as a crucial practice location in the 21st century. Factors that will drive an increasing need for wellness-related services are based upon a collecting body of clinical evidence that an individual's health is directly associated to physical in addition to emotional well-being. What is a single payer health care system. Aspects that will increase the need for services in this location consist of a growing aging population with increased longevity; an increased focus on health care variations impacting treatment and services; the health effects of rising rates of weight problems; and factors that challenge the quality and pace of life, including innovation and imbalances in life functions.
How Long Do You Have Health Insurance After Leaving A Job? Can Be Fun For Everyone
The Practitioner Wellness page supplies resources and standards to attend to professional well-being and provide tools for coping. We hope the resources below will assist you in your practice. If you have extra concerns, try publishing them on Commun, OT, a neighborhood for occupational treatment practitioners similar to you. If you are an AOTA member, you are currently joined Commun, OT! Simply use your member login and password for the AOTA Web site to gain access to Commun, OT. Developed for OT professionals and other experts to explain the function and scope of occupational therapy. Find our truth sheets here. Read the SIS Quarterly Practice Connections articles associated to Health & Wellness.
AOTA Members: $259, Nonmembers: $359 Earn. 25 CEU (3. 13 NBCOT PDUs/2. 5 contact hours). AOTA Members: $68, Nonmembers: $97.
The terms health and wellness are typically tossed together, thanks in big part to the prevalence of health cares promoting better health in the workplace. It's easy to see how the 2 terms might be interchangeable, but the difference between health and health is necessary. Health care mainly focus on the idea of preventative care, which is mostly created to conserve insurance policy holders (and employers) cash in the long run. Although numerous employers can regrettably sink a load of time and cash into wellness programs without any strategy whatsoever. The basic idea is that if people are getting regular checkups, sticking to their prescribed medication program, and getting advised vaccines, illness can either be totally prevented, or a minimum of managed before they end up being extraordinarily pricey.
/cdn.vox-cdn.com/uploads/chorus_asset/file/15988428/1138451056.jpg.jpg)
So let's dive into this difference and why it matters. According to the World Health Company, "Health is a state of complete physical, mental and social wellness and not merely the absence of disease or infirmity." To put it simply, your health has to do with a lot more than physical ailments it has to do with psychological and social fitness, too. On the other hand, health is the "active procedure of ending up being aware of and making choices towards a healthy and fulfilling life. [...] a dynamic procedure of modification and growth." The two principles are not revers, but rather go together in one's mission toward complete wellness.
Health is the action while (excellent) health is the preferred outcome. We can't always select the state of our health. High cholesterol and blood pressure are largely genetic. People are born with heart problem and a predisposition towards diabetes. Mishaps trigger injuries that last a lifetime. However health, on the other hand, is an option. We can pick to work out routinely to handle our health conditions (where possible). We can choose to quit cigarette smoking and to take our medications as prescribed. We can see a therapist when our mindset needs some assistance. Health is a way for us to actively pursue better health. What is universal health care.
Which Of The Following Is A True Statement About The Effects Of Stis On One's Health? Can Be Fun For Anyone
Even though none of us will ever be in "best" health, making a conscious effort to improve our wellness can make us feel better and eventually, cost us less money in health care expenses down the line. For companies, understanding the distinction in between health and http://josuecjlk861.raidersfanteamshop.com/how-what-countries-have-universal-health-care-can-save-you-time-stress-and-money wellness is necessary because it notifies the corporate communications you have with your workforce - How does health insurance deductible work. Lots of people wish to live much healthier lives, but aren't sure of how to tackle it. Taking this chance to inform them about health and how simple way of life changes like substituting soda for water, taking a walk during breaks rather of sitting, and loading a lunch rather of purchasing out can help people attain their health goals.
For example, rather than informing your labor force on healthy consuming in basic, acknowledge that your workforce sometimes goes out to lunch. Discover the ten most frequented dining establishments around your office and educate employees on the healthiest menu items at each establishment. Another example would be to draw up a number of lunchtime walking loops of different girths your workplace, rather than just reminding your workforce of the Learn more benefits of walking. The lower your workers' health dangers, the much better they'll feel. This positive shift has a trickle-down effect for you as healthy workers utilize less ill time, resulting in increased productivity. In addition, the lower the risk pool, the more stable your health care expenses will become.
AboutExcitement About What Is An Underlying Health Condition
Nature of work requires regular physical effort and handbook mastery with periodic direct exposure to accident and health hazards and disagreeable elements when conducting or reviewing field examinations. This is the principal-level class in the Environmental Health Inspector series. It is differentiated from the 6122 Senior Citizen Environmental Health Inspector in that the 6124 has higher supervisory responsibility and manages the most complicated and hard examinations (What is a health coach). According to Civil Service Commission Guideline 109, the responsibilities specified listed below are representative of the series of tasks designated to this task code/class and are not planned to be an inclusive http://lorenzolsgz624.almoheet-travel.com/the-greatest-guide-to-how-to-cancel-health-insurance list. 1. Administers and is directly responsible for the work assignments and efficiency of a Senior Environmental Inspector, inspectors and auxiliary workplace and clerical workers; reviews reports and findings of inspectors; interprets suitable laws, ordinances, regulations and recognized policies and treatments.
Administers the investigation of complaints including all structures; takes needed action to ease off unlawful health, hygienic and security conditions; coordinates efforts with appropriate city departments in the enforcement of the building, electrical, plumbing, fire and police codes; appears as witness in court litigation when required and testifies in cases including food establishments, real estate, industrial buildings, dangerous products and waste facilities and other matters, 3. Administers the conduct of complaint inspections of residences, hotels, apartment homes, and other numerous residences, relative to sanitation, general upkeep of structural and operational features, light, ventilation, usage and tenancy, security and for compliance with suitable codes, discovers violations; collaborates efforts with the appropriate city department in the enforcement of the building, electrical, plumbing, fire and police codes, makes follow-up examinations to guarantee bought corrections have actually been made; makes recommendations for order of trip or condemnation of buildings staying in violation; prepares condemnation reports, appears and testifies at condemnation hearings.
Prepares work schedules and projects for workplace and field activities, investigations and unique surveys relating to food, real estate, urban renewal, industrial health, air contamination, vector control, mosquito control and abatement, harmful products management and other ecological, eco-friendly issues; observes regular workplace treatments and field activities for purposes of improving kinds, techniques and overall efficiency; helps in the advancement and development of subordinates through training and effective use of staff member advancement program, 5. Conducts area evaluations to determine performance of inspection work; confers with workers on all problems worrying both office and field activities; recommends on finest procedures in order to insure optimal degree of compliance - What is health literacy.
Talk to outdoors individuals and agents of various issues and facilities regarding compliance with regulative requirements and orders released, and to work out disagreements or misconceptions of existing provisions; consults architects, professionals and attorneys on strategies and requirements for new structures or rehab of existing structures; consults members of other governmental jurisdictions in matters associating with specific activities and analyses of appropriate codes and policies; accompanies agents of the State Department of Agriculture on field assessments of meat processing plants. 7. May be designated to administer and supervise the advancement and implementation of programs with regard to health and wellness for workers of the Health Department; examines and triggers compliance with joint commission accreditation and associated requirements for organizations and other centers of the Health Department; personally reviews and might investigate reports of threats or injuries along with corrections for same; coordinates the mishap prevention program for the department; offers technical info and guidance to supervisory personnel; and normally offers an awareness for safe working conditions and correction of safety risks amongst city employees.
The Best Strategy To Use For How To Find Health Insurance
Personally carries out investigations of an extremely important or special nature straight concerning department policy and on matters needing more knowledgeable judgment. 9. Makes last suggestions for issuance of warrants, citations and of any more action required to protect compliance with local, state or other existing guidelines; makes last recommendations for condemnation of homes when owners stop working to adhere to statutory requirements; participates in condemnation hearings and court lawsuits in connection with specific charges and Substance Abuse Center violations; workouts independent judgment in quarantining and condemning unsatisfactory foods items. 10. Reviews reports of finished work assignments of both field and office activities; prepares regular combined reports of district ecological health inspectors; carries out periodic staff conference for function of sharing brand-new information and explanation of existing requirements, policies, methods and treatments; analyzes reports and activities of office and clerical workers for compliance of necessary information and analytical data.
Functions as departmental agent in matters associating with safety and mishap prevention; carries out safety meetings with supervisorial workers to evaluate employee accidents and accident reporting along with mishap prevention. 12. When designated, supervises and works as specialist for the Elder Environmental Health Inspector in charge of dairy and milk sanitation expert for district offices of the bureau of environmental health. Needs a broad working understanding of: Field inspection strategies and treatments and associated workplace routines, types, files and reports; state laws and city ordinances and health department guidelines and guidelines relating to general sanitation, real estate evaluation, hospital procedures and sanitation, mishap prevention and security procedures.
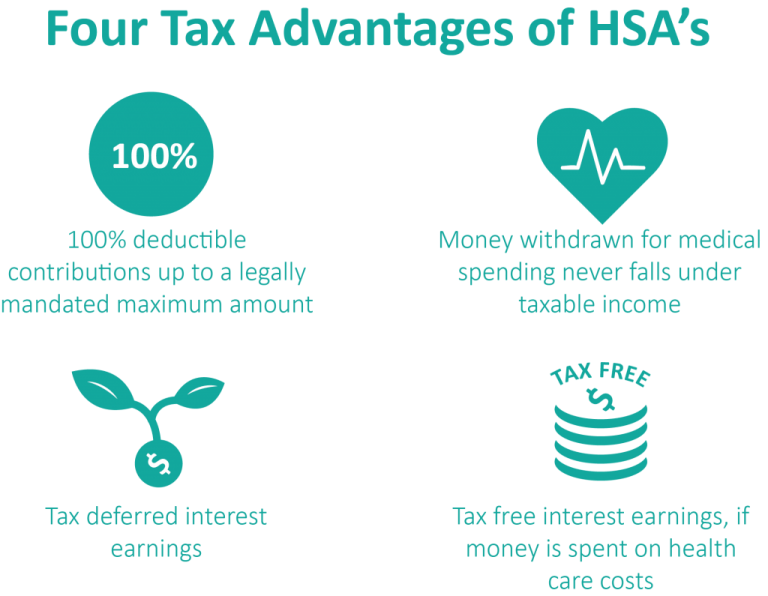
These minimum qualifications establish the education, training, experience, unique skills and/or license( s) which are needed for work in the classification. Please note, additional certifications (i. e., special conditions) may use to a particular position and will be specified on the exam/job statement. Education:: Possession of a baccalaureate degree from a recognized college or university in engineering, environmental health, mathematics, or physical, natural or life sciences. Experience:: Needs 7 (7) years of experience in harmful products, contaminated materials, site mitigation and/or medical waste as a professional or inspector in an environmental health company or associated regulatory/service company, or as an expert expert in the ecological health market; Five (5) year of experience as an inspector in a Certified Unified Program Company (CUPA).
License and Accreditation:: Needs belongings of a REHS (Registered Environmental Health Professional) Certificate, Check out here provided by the State of California Department of Health Providers and eligibility to be deputized as a peace officer.: Requires a CA UST Inspector Accreditation issued by the International Code Council (ICC) and possession of an existing HAZWOPER Certification.: Require belongings of a legitimate California driver's license. All City and County of San Francisco staff members are designated Disaster Service Workers through state and regional law (California Federal government Code Section 3100-3109). Employment with the City needs the affirmation of a commitment oath to this result.
AboutExamine This Report about What The Health Facts
Calling their bluff, the New Democratic Partya social-democratic opposition partyhas revealed that it would introduce an expense in Parliament to freeze drug prices and execute a national, universal pharmacare program by the end of the year. The NDP would face an uphill fight: The legislation would have a slim chance at passing without the Liberals' support, and they are confronted with a slate of Conservative provincial leaders who are hostile to the idea.
Referrals to Canada turn up in in fiery op-eds both for and against implementing a single-payer system, as well as on the campaign path, as Democratic prospects have actually been pushed to articulate their positions on health care. Simply last summer, Bernie Sanders took a bus journey across the border with a group of Americans who have type 1 diabetes, in order to acquire cheaper insulin.
6 million times. This rosy view does Get more info not show the impact of the Canadian system on somebody like Burdge, who has actually ended up being an outspoken advocate for pharmacare. "For folks like myself who are managing a complex chronic illness, where we have to be injecting ourselves with drugsthe financial problem of that causes more stress and makes us sicker," she says, explaining that Canada's absence of pharmacare likewise avoids people from accessing brand-new medical devices and treatments.
Excitement About Which Of These Is The Definition Of Palliative Care According To The World Health Organization?
That's never the case, in my experience." The creator of Canadian medicare never ever meant for it to be by doing this - who led the reform efforts for mental health care in the united states?. Tommy Douglas, a democratic socialist who was premier of Saskatchewan prior to ending up being the first leader of the NDP, fought intensely to instill his vision of an extensive system that would cover every Canadian.
By the mid-1950s, rising hospital costs across the country spurred popular assistance for federal intervention, and the federal government soon concurred to offer joint funding for universal health center insurance programs. When Douglas was up for reelection in 1960, he announced that his provincial government would expand the program to cover doctor services and clinic check outs.
( The American Medical Associationthe very same association that is fighting single-payer in the United States nowalso moneyed the Saskatchewan anti-medicare campaign.) The anti-medicare lobby fought to protect the private insurance market and maintain a fee-for-service system, decrying medicare as "socialized medicine" and flooding regional airwaves and newspapers with propaganda that varied from threatening (medical professionals will leave the province en masse!) to ludicrous (medicare might institute obligatory abortion).
Some Known Facts About Why Doesn't The Us Have Universal Health Care.
Entrepreneur, conservative activists, and popular physicians continued to assault medicare; some burnt effigies of Douglas in the streets and characterized government leaders as Nazis. But the Saskatchewan federal government declined to give up, and with the assistance of a British arbitrator, brought the doctor's strike to an end 23 days later on.
That Saskatchewan was among the poorest provinces in the country at the time shows federal governments "don't need to be wealthy [they] need the combination of political management and grassroots support to get this done," states Dr. Joel Lexchin of Canadian Physicians for Medicare, a national advocacy group that opposes the privatization of Canada's healthcare system.
Eventually, the Canadian federal government would begin to provide joint financing for this too, needing all provinces and areas getting federal money to ensure their medicare programs met 5 requirements: public administration, ease of access, comprehensiveness, universality, and mobility. Today, Canadians can walk into a physician's office, center, or hospital throughout the country and receive care with very little to no co-pays, deductibles, or charges.
Hop over to this website >The Facts About What Is Required In The Florida Employee Health Care Access Act? Revealed
He saw medicare as the first stepto be followed by universal coverage for dental, vision, drugs, long-term and house care, and mental health support. Rather, he invested the last decades of his life fighting the sluggish creep of private insurance coverage plans and billing practices that threatened to produce a two-tier system.
Spending plan cuts and austerity policies under successive Conservative and Liberal governments through the 1990s and 2000s additional destabilized medicare, striking Very first Nations and Inuit neighborhoods, front-line healthcare employees, refugees, and working-class people hardest. Canada's latest Conservative prime minister, Stephen Harper, was a vocal challenger of universal health care and openly encouraged privatization: His party declined to keep track of provinces' compliance with the 5 requirements for financing and slashed the federal government's share of health spending by $36 billion over a decade.
( Trudeau's Liberals campaigned on a pledge to reverse these financing cuts. They haven't done that.) Prescription drugs play huge function in healthcare: Around half of all Canadian adults now take a prescription medicine frequently, and approximately two-thirds of Canadians aged 65 and up are recommended five or more everyday medications - who is eligible for care within the veterans health administration.
Some Of How Much Is The Health Care Penalty
Only individuals in the United States and Switzerland invest more per capita. The existing systemin which medicare just covers drugs administered at hospitalshas presented ridiculous loopholes. "I know some diabetics who will just stroll into emergency to get their insulin, due to the fact that one part of the system remains in location, but the other part of it is not," says Burdge.
The federal government covers registered First Nations and Inuit communities, and provinces and territories usually guarantee that "devastating" drug expenses are covered for everyone. However the large majority of working-age grownups are delegated pay for prescriptions out-of-pocket, or pay into private strategies provided by their employerswhich is hard, when the really capitalist reasoning that has chipped away at medicare has actually also fueled the increase of precarious, gig-economy tasks.
Danny, who lives in British Columbia, is amongst the approximately 1 million Canadians who must cut back on groceries or decline the thermostat to manage prescription drugs. (He asked The Nation not to share his last name.) After Danny had tried more than a dozen different antidepressant medicationssome with crippling side effectsand sustained 2 prolonged psychiatric hospitalizations, his doctor offered him samples of an antidepressant that he refers to as "the first medication that has done anything for me (how is canadian health care funded)." But his present insurance coverage, a private plan he pays into through a company, will not cover the drug.
3 Simple Techniques For Which Type Of Health Care Facility Employs The Most People In The U.s.?
There isn't a generic variation of Danny's medication on the market, and BC's drug expenses are http://johnnydfsg690.image-perth.org/the-of-what-are-the-health-benefits-of-turmeric considered to be among the worst in the country; the out-of-pocket price is expensive. "I'm devastated," says Danny. "I've spent the last couple of days sobbing about it." Ninety-one percent of Canadians support national pharmacare, according to one poll.
( The NDP has said its bill will follow the 2019 report's suggestions.) Pharmacare would conserve Canadians more than CAD 4 billion (about $3 billion) each year, consisting of CAD 1. 2 billion ($ 900 million) simply from cutting back on unnecessary emergency sees and hospitalizations. So why can't Canada get it done? If there's something the American and Canadian governments share, it's their fealty to Big Pharma.
Private insurance intermediaries negotiate with drug business rather. Conditions are various in Canada, but drug business still have a stranglehold on political action there. As medication rates have skyrocketed over the previous years, so have Big Pharma lobby sees to Canadian politicians and medical professionals. Since 2006, the number of drugs that cost more than CAD 10,000 (about $7,500) per year has more than tripled.